This method of anesthesia for the rat, and positioning and restraint of the hind limb for in vivo µCT imaging facilitates the acquisition of high quality images appropriate for the analysis of tibia micro-architecture. Proper positioning of the rat hind limb involves the leg being fully extended and the entire foot and ankle restrained in foam (Figure 1A) resulting in an acquired image of sufficient quality for analysis of the trabecular and cortical micro-architecture (Figure 1B). Insufficient placement and restraint of the hind limb (Figure 1C) can result in images with movement artifacts (Figure 1D), while a tail that is not fully removed from the scanning field of view (Figure 1E) will interfere with X-ray attenuation by the scanned samples (Figure 1F) and alter BMD and tissue mineral density (TMD) measurements. Either of these placement errors will result in a poor-quality scan that should not be further analyzed. Attaining images of poor quality will alter the quantification of the fine trabecular network and cortical structure of the hind limb and will produce inappropriate or inconclusive data14.

Figure 1. Representative images of placement of the rat hind limb and corresponding acquired images of the proximal tibia in cross-section.
(A) Proper placement of the rat hind limb with the ankle fully restrained in foam, leg extended and tail pulled away from the tibia provides sufficient image quality in (B) cross-section of the tibia and its trabecular and cortical micro-architecture. (C) Improper placement of the rat hind limb with the leg not fully extended and ankle not fully restrained in foam may result in (D) movement artifacts, seen as streaking in cross-section. (E) Objects interfering with the field of view, such as the tail not pulled away from the tibia (F) interferes with x-ray attenuation from the tibia and can result in altered BMD and TMD measurements, although not visually evident. The bottom left corner in panel F shows a portion of tail in the field of view, that interfered with the x-ray beam that subsequently passed through the tibia. Red dotted lines in the left panels indicate the cross section presented on the right panels. Please click here to view a larger version of this figure.
Supplementary Figure 1. Isoflurane anesthetic unit. Isoflurane anesthetic unit set up to provide 3-4% isoflurane dissolved in O2 at a continuous flow-rate of 1-2 L/min for induction of general anesthesia. Please click here to download this figure.
Supplementary Figure 2. Ensuring depth of anesthesia. Measure pedal reflexes by pinching the toes of the rat receiving continuous inhaled anesthetic through a face mask or nose cone. The pain response is more evident when the leg is slightly extended. Very strong pinches or the use of forceps or clamps can induce tissue damage and therefore should not be used. Please click here to download this figure.
Supplementary Figure 3. Screen capture of the live-feed physiological monitoring camera view. Please click here to download this figure.
Supplementary Figure 4. Rat laying in the supine position on the carbon-fiber scanner bed. Please click here to download this figure.
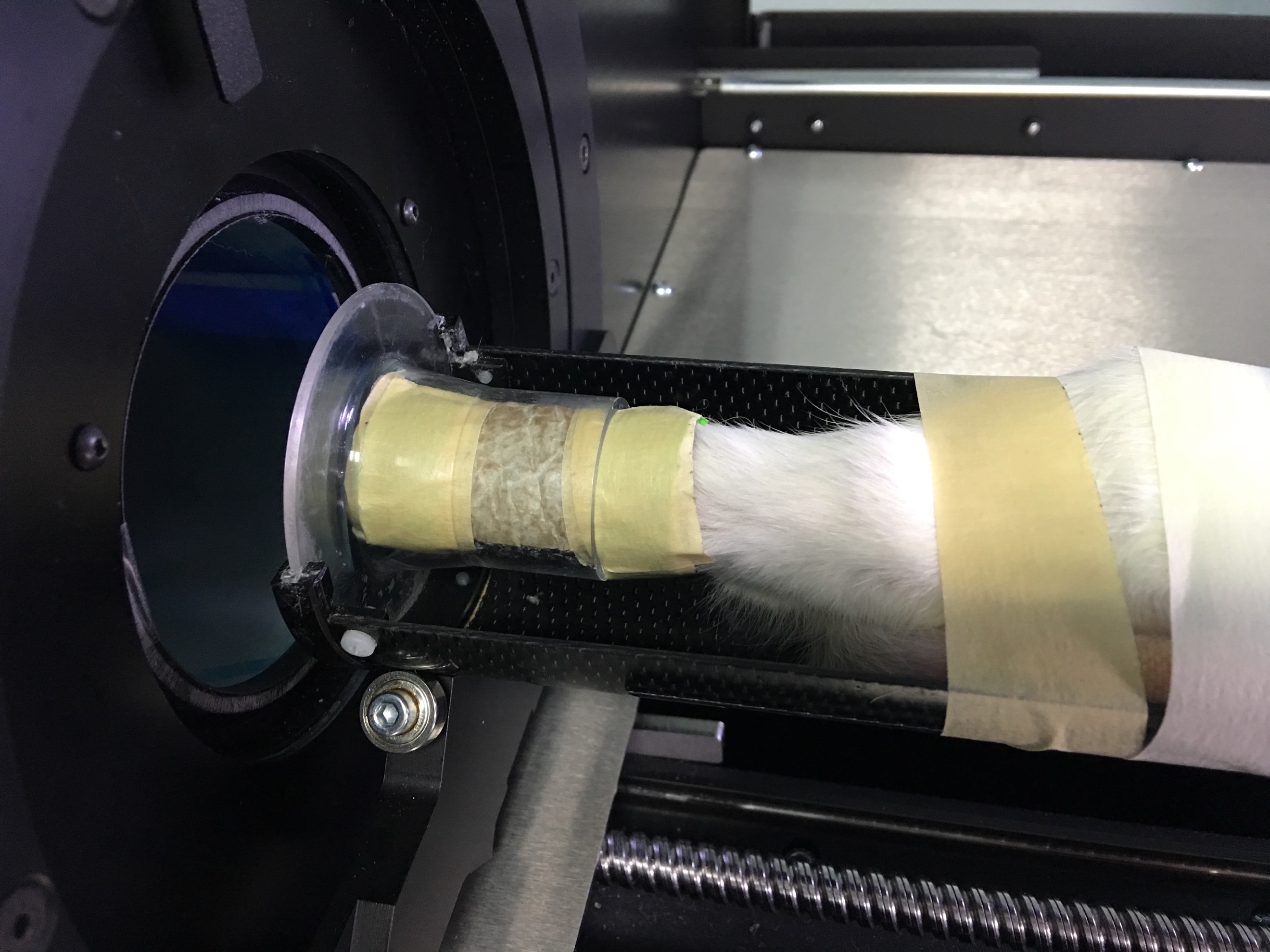
Supplementary Figure 5. Right foot of the rat restrained in a malleable foam tube. Right foot of the rat is restrained in a malleable foam tube with the toes extending out of the tube (not pictured here). The foam tube is restrained in a plastic holder (please refer to Table of Specific Materials/Equipment for more detailed information). Please click here to download this figure.
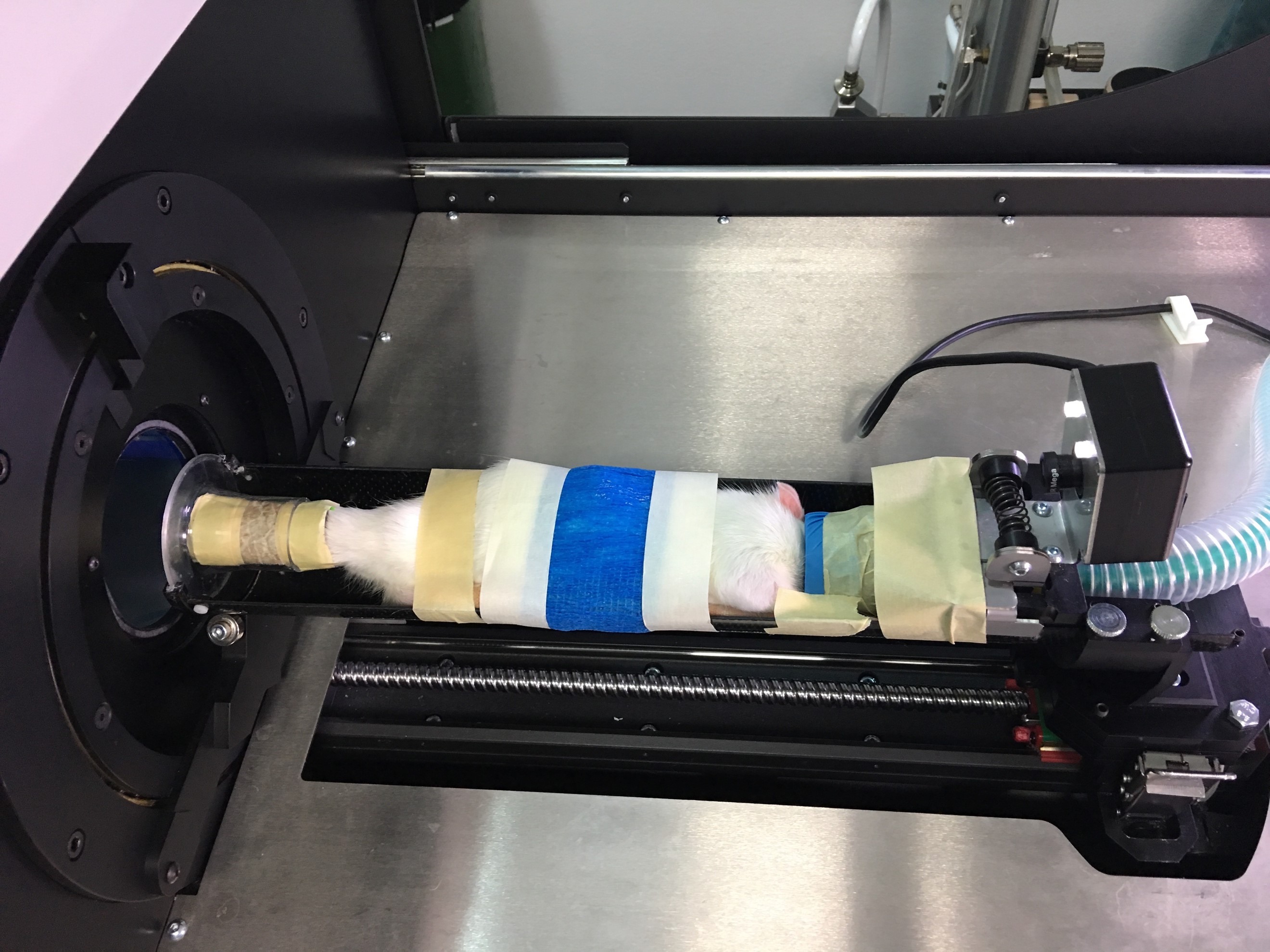
Supplementary Figure 6. Rat secured in position with the right leg extended straight. The tail and left foot is taped away from the right leg (toward the torso), the hips are secured and the rat torso is wrapped in vet-wrap (blue) to limit heat loss. Please click here to download this figure.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}