The prone position of the pig's head provides optimal access for the surgeon during the procedure, and the use of stabilizing sandbags reduces the risk of unintended shifts in the pig's head position while drilling.
During this demonstration, the superficial anatomical landmarks of the pig's superior skull (both superior orbital crests and the nuchal crest) (Figure 1 and Figure 3) were used to precisely identify the centered sagittal line before making the incision. After the incision and removal of the galea aponeurotica, the sagittal suture was identified to determine the true anatomical midline (Figure 2). Following exposure of the frontal bone, the three palpable landmarks (Figure 1 and Figure 3) and the sagittal suture (Figure 2) were used to define a triangle within which the borders of the craniectomy were determined within the desired location (Figure 4A). These landmarks are well-suited for this procedure as they are closely related to the pig brain (Figure 7).
After gradually drilling and thinning the frontal bone along the borders of the craniectomy (Figure 4B), a contact point for the underlying dura mater was achieved, allowing for assessment of the remaining thickness of the frontal bone.
Finally, after carefully removing the frontal bone, the underlying dura mater covering the cranial two-thirds of both cerebral hemispheres was revealed. The procedure was considered successful because (1) the revealed underlying dura mater was intact (Figure 6); (2) the opening in the frontal bone was centered, confirmed by the location of the dorsal sagittal sinus (Figure 5); and (3) only minor venous hemorrhages occurred along the exposed spongiosa bone.
The integrity of the dura mater was assessed by visually inspecting for obvious cerebrospinal fluid (CSF) leakage through smaller defects. These leaks would pulsate synchronously with the pulsation of both hemispheres. The intact dura mater was confirmed as no visual CSF leakage was observed, and both hemispheres appeared elevated and rounded synchronously with the pulsation (Figure 6). This elevated appearance of the hemispheres indicates a net positive pressure within the CSF, equivalent to intact meninges.
The correct centered location of the craniectomy was crucial for several reasons. Firstly, it ensured maximal exposure of both hemispheres for later instrumentalization. Secondly, it reduced the risk of accidentally damaging the dorsal sagittal sinus with the drill. The correct location was confirmed after the bone plate was removed, and the contours of both cerebral hemispheres were symmetrically separated by the fissure just above the dorsal sagittal sinus (Figure 4).
Minor venous bleeding is expected from both the dura mater and the exposed trabecular bone. This can be managed by applying bone dust from the craniectomy for a few minutes to achieve hemostasis. If this is not sufficient, hemostasis can be ensured by applying low-voltage cauterization to the origin of the hemorrhage using a mono- or bipolar cautery.

Figure 1: Image of the exposed frontal bone. The three anatomical landmarks are identified by manual palpation: the nuchal prominence and the caudal aspect of each superior orbital crest. Please click here to view a larger version of this figure.

Figure 2: Image of the exposed frontal bone after dissection, revealing the sagittal suture and the coronal suture. Please click here to view a larger version of this figure.

Figure 3: 3-dimensional computed tomography scan. The scan of the posterior aspect of the porcine skull visualized from a frontolateral perspective (A) and a posteriosuperior perspective (B). Anatomical landmarks of the frontal bone are highlighted in red (superior orbital crest) and blue (nuchal crest). Please click here to view a larger version of this figure.
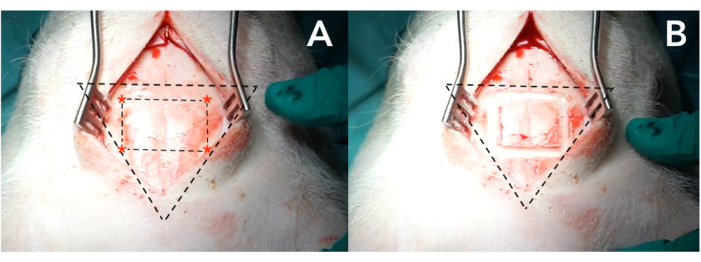
Figure 4: Images of the exposed frontal bone. (A) Defining each corner of the rectangular craniectomy using the nuchal prominence and superior orbital crests as landmarks. (B) Drilling the initial line of the craniectomy by connecting each corner. Please click here to view a larger version of this figure.

Figure 5: Depiction of the exposed dura mater with underlying cerebral hemispheres and sagittal suture. Please click here to view a larger version of this figure.

Figure 6: Image of the dura mater with underlying cerebral hemispheres seen from a frontal perspective. If the dura mater is intact, both hemispheres are elevated and rounded synchronously to the pulsation (marked with white stipulated lines). Please click here to view a larger version of this figure.

Figure 7: Horizontal computed tomography scan. The scan of the porcine skull revealing the anatomical relationship between the posterior orbital crest (red), nuchal crest (blue), and cerebrum (yellow). Please click here to view a larger version of this figure.
