The complete dacryoadenectomy method described here was performed on 8 animals. It requires a moderate degree of surgical skill. Surgical time averaged about 2.2 h for bilateral surgery, excluding the removal of the nictitating membrane, which was done separately and required <10 minutes. There were no fatalities or intraoperative complications and no rabbit required any hemostatic aid other than modest cautery.
Our surgical approach successfully induced dry eye in all eyes. This was confirmed by a panel of clinical and laboratory markers of DED (Table 1). During the 8 weeks of observation, the mean TBUT was suppressed by more than 75% of preoperative levels (p < 0.0001 for all time points). Similarly, the Schirmer's tear test decreased by approximately 50%, remaining so for the 8 weeks of observation; it showed no trend for recovery during the follow up period. Postoperatively, tear osmolarity showed a 10% increase consistent with DED, sustained for at least 8 weeks postoperatively. Rose bengal staining of the cornea also increased and did not show signs of recovery during the 8 weeks of follow-up (Figure 8). All eyes undergoing complete dacryoadenectomy showed marked reduction in goblet cell numbers and epithelial changes consistent with dry eye (conjunctival impression cytology).
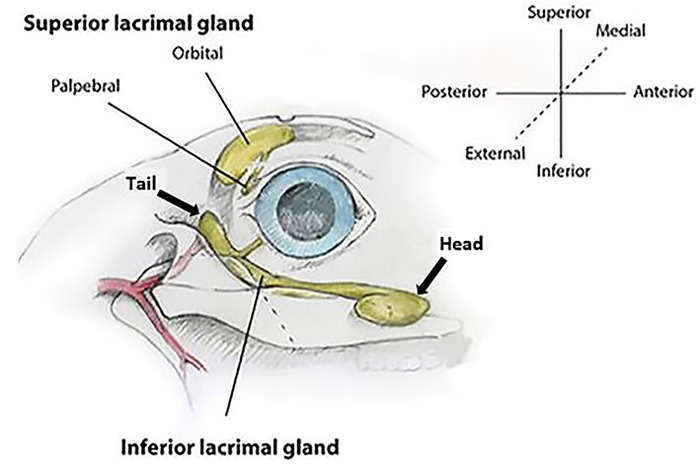
Figure 1: Rabbit lacrimal gland anatomy (right eye). The orbital superior lacrimal gland (OSLG) is comprised of a larger orbital part and smaller palpebral component. The larger inferior lacrimal gland (ILG) is comprised of the anterior/head and posterior/tail portions. Coordinate axes show the terminology used for all descriptions of orientation used within the text. Please click here to view a larger version of this figure.
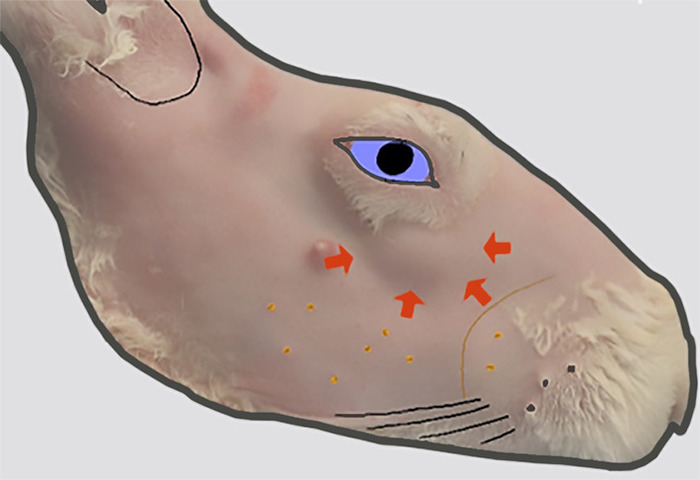
Figure 2: Location of the head of the ILG. The lateral view of the right face after removal of fur. A bulge in the skin contour (indicated by thick arrows) inferior to the anterior orbit indicates the location of the head of the ILG that lies on the external surface of the zygomatic bone at this location. Please click here to view a larger version of this figure.
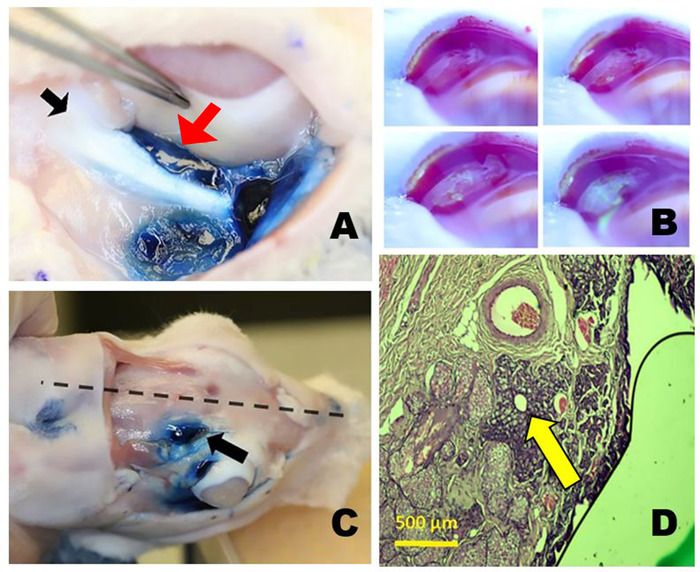
Figure 3: The orbital lacrimal glands. (A) The right inferior lacrimal gland (ILG) after staining with Evans blue dye showing the close proximity of the tail of the ILG (red arrow) just medial to the zygomatic bone (black arrow) and inferior to the globe. (B) Tear production from the palpebral superior lacrimal gland (PSLG). Time-lapse photos taken after topical application of 2% fluorescein. Aqueous fluid emanating from the PSLG dilutes the initially dark blue or black fluorescein dye turning it bright yellow green (similar to Seidel testing). (C) Position of orbital SLG (OSLG) in the rabbit skull, lying close to the midline of the skull (dotted line) within the posterior incisure (arrow). Evans blue dye was injected into the OSLG and palpebral superior lacrimal gland. (D) Histology section through the main excretory duct of the OSLG surrounded by a small amount of glandular tissue (arrow) is seen in this histopathologic cross-section stained with hematoxylin and eosin dyes taken through the posterior (temporal) aspect of the upper right eyelid. Please click here to view a larger version of this figure.
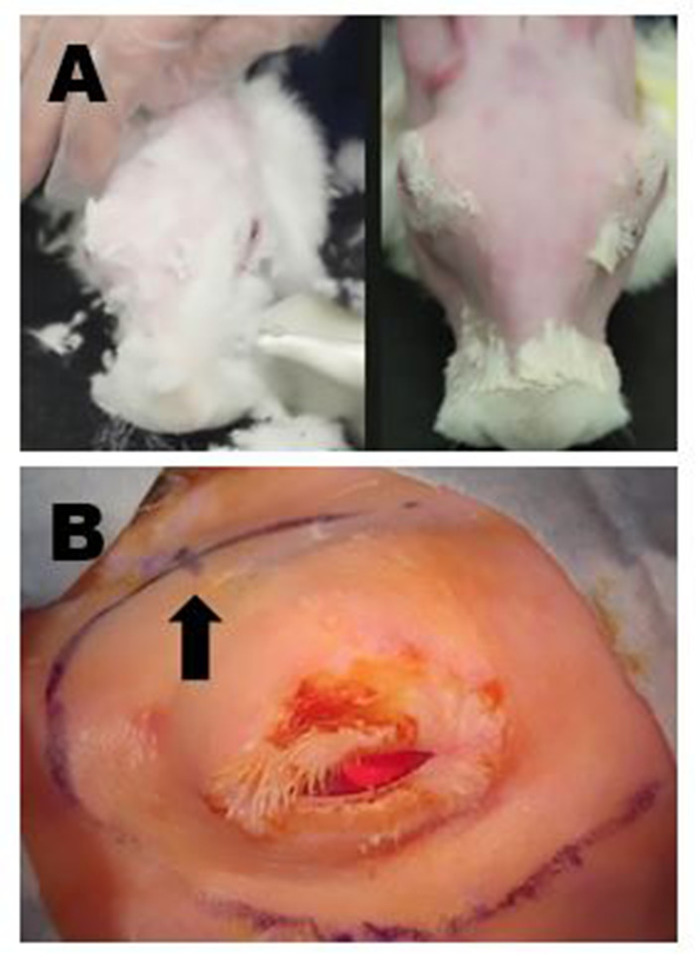
Figure 4: Surgical site preparation. (A) Upper left panel: Removal of long fur with shears. All residual fine fur is subsequently removed with a mild depilatory cream. Upper right panel: Final appearance following complete fur removal that allows for surgical marking and high-quality ultrasound of the ILG to be performed. (B) Appropriate surgical markings of the right periorbital region are shown; in this example, the incisions to remove the OSLG and ILG have been connected to create one long curvilinear incision. The location of the posterior incisure is indicated by a small hash mark on the curvilinear incision site marking (arrow). Please click here to view a larger version of this figure.
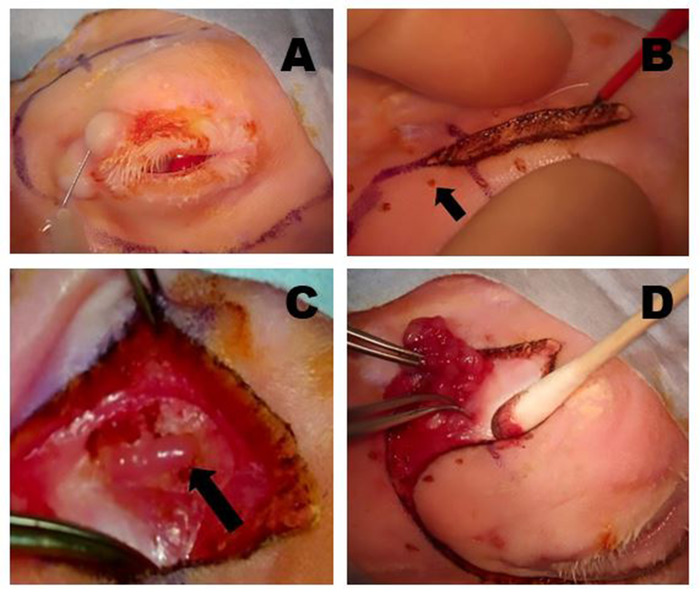
Figure 5: Removal of the OSLG. (A) Surgical sites are infiltrated with anesthetic using a 50:50 combination of 2% lidocaine with 1:100,000 epinephrine and 0.5% bupivacaine, which is injected into the upper lid and along the incision lines to minimize discomfort during the procedure. (B) A Colorado microdissection needle is used to incise the skin and superficial muscle layers along the pre-marked surgical incision sites. Gentle traction across the wound is applied to help create the dissection plane. The small pinpoint burns (arrow) were made with the Colorado needle at equidistant points along the incision line to help optimally realign the tissues during wound closure. (C) The OSLG is exposed after tissues overlying the posterior incisure have been mobilized (arrow). The capsule of the gland has been incised. The OSLG can be prolapsed by applying medial pressure to the globe facilitating its removal. (D) Forceps are used to engage the OSLG and gently remove it from its deeper position within the orbit through the posterior incisure. Please click here to view a larger version of this figure.
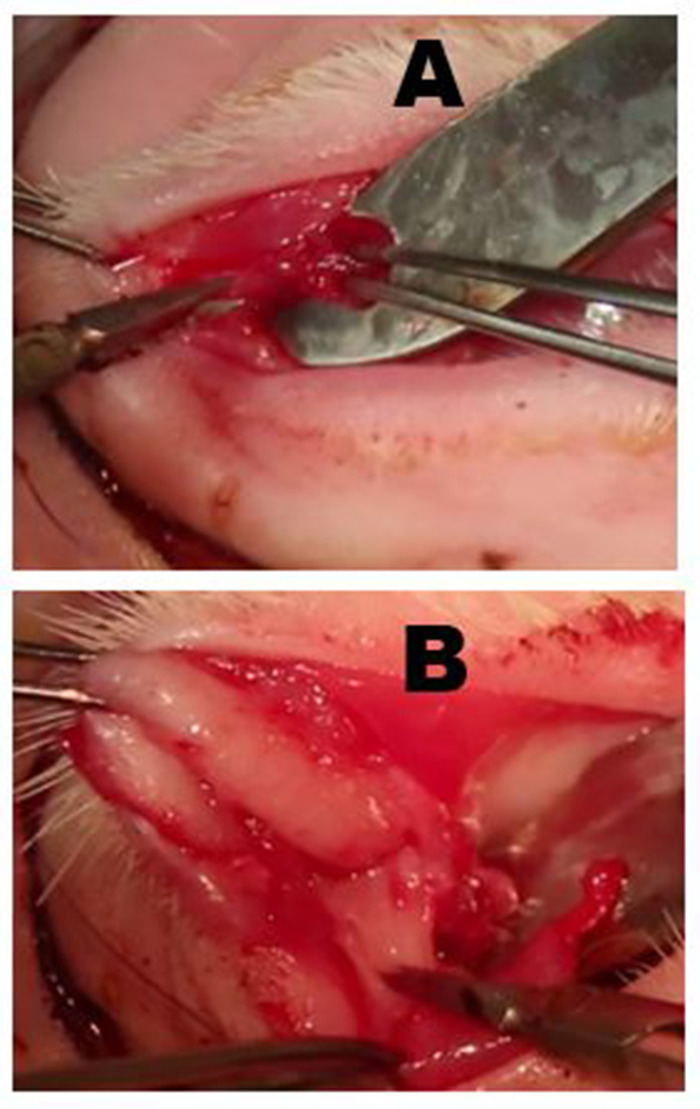
Figure 6: Removal of the palpebral superior lacrimal gland (PSLG) and excretory duct. (A) Following eversion of the upper eyelid, the bulbous portion of the PSLG is engaged with forceps and dissected off the tarsus using scissors. Traction applied to the PSLG with forceps is critical to maintaining the surgical plane. (B) The dissection of the PSLG and the main lacrimal duct is carried superiorly toward the orbital rim using sharp dissection and continuous traction on the gland and duct tissues to maintain the appropriate surgical plane. The dissection should proceed to the point where the OSLG was removed. Please click here to view a larger version of this figure.
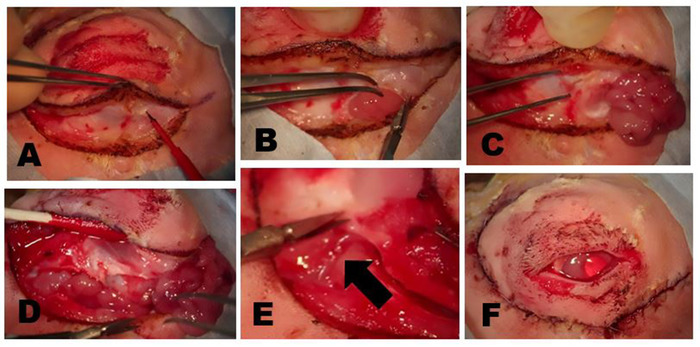
Figure 7: Removal of the ILG. (A) The skin and superficial muscle are incised until the fascial plane overlying the zygomatic bone or superficial part of the masseter muscle is reached. The head of the ILG usually is clearly evident as a small bulge located under the anterior limbus. (B) The fibrous capsule of the ILG is incised with scissors exposing the ILG. Once the capsule is incised, the deeper portions of the gland can be easily removed. (C) The most external portion of the ILG head that lies on the zygomatic bone has been exposed and reflected anteriorly showing the underlying zygomatic bone. (D) Incision of the orbital septum along the inferior rim exposes the tail of the ILG. (E) A branch of the external carotid artery feeds the tail of the ILG (arrow). (F) Appearance following the closure of skin incisions after complete dacryoadenectomy. Please click here to view a larger version of this figure.
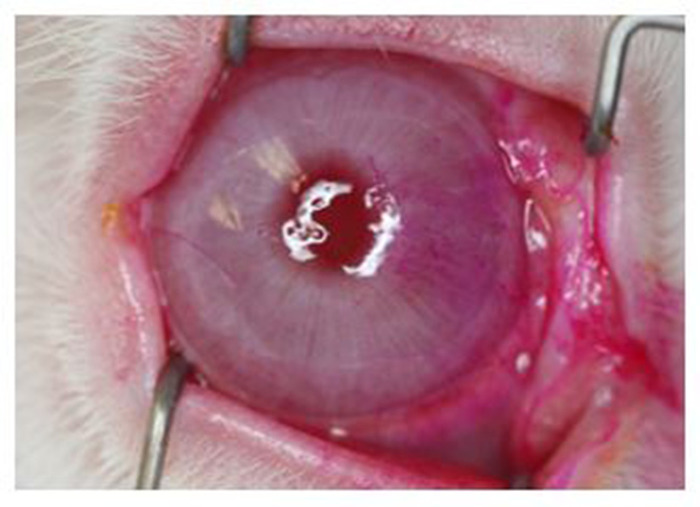
Figure 8: Rose Bengal staining of the corneal surface. External photograph showing prominent staining, most notable on the nasal quadrant. All eyes undergoing complete dacryoadenectomy developed similar changes that were evident by 1 week after surgery and persisted for at least 6 weeks. Of note, the light reflex from the ring flash shows distortion from a dry ocular surface demonstrating how dry eye can adversely impact vision. Please click here to view a larger version of this figure.
| Dacryoadenectomy | ||
| mean ± SEM; n = 16 eyes | ||
| Baseline | Week 2 | |
| Tear break-up time, s | 60.0 ± 0.0 | 4.5 ± 1.2 |
| p < 0.0001 | ||
| Tear osmolarity, mOsm | 291.2 ± 3.7 | 315.3 ± 5.5 |
| p = 0.001 | ||
| Schirmer tear test, mm | 18.3 ± 1.3 | 10.5 ± 1.6 |
| p = 0.0006 | ||
| Rose bengal, modified NEI score | 0.0 ± 0.0 | 4.28 ± 0.6 |
| p < 0.0001 | ||
| Operated vs. baseline: Dacryoadenectomy: TBUT, p < 0.0001; tear osmolarity, p < 0.001; Schirmer tear test, p < 0.0006); and rose bengal. | ||
Table 1: Dry eye parameters on postoperative week 2.
