LDPI was used to measure BF in the spinal cord, which was quantified along the rostral-caudal axis of the spinal cord by extracting linear profiles (Figure 4). Figure 5A and Figure 5B represent the flux imaging of the spinal cord of the sham group and SCI group, respectively. Figure 5C and Figure 5D represent the altering BF along the rostral-caudal axis of the spinal cord of sham group and SCI group, respectively. A comparison of Figure 5A and Figure 5B demonstrated that SCI induced reduction of BF, and BF of the epicenter was lower than rostral cord and caudal cord.
LDPM showed the time-domain LD signal and SO2 and Figure 6 illustrated the acquiring and processing of the LDPM data. After the data were recorded, an 8 min stretch of continuous Region of Interest (ROI) data was selected, which was then filtered by a built-in filter to minimize any non-biological signals. Subsequently, the ROI was statistically analyzed and the results were exported in a raw data format. Figure 7 recorded the periodic variation of BF and SO2 over time in the sham group and SCI group. As shown in Figure 7A, the spinal cord BF of the SCI group significantly decreased compared with the sham group. Simultaneously, the SO2 of the spinal cord was remarkably lower after spinal cord concussion (Figure 7B), which was consistent with the change of BF after injury. To reduce disturbance, measurements were taken repeatedly and the data were normalized.
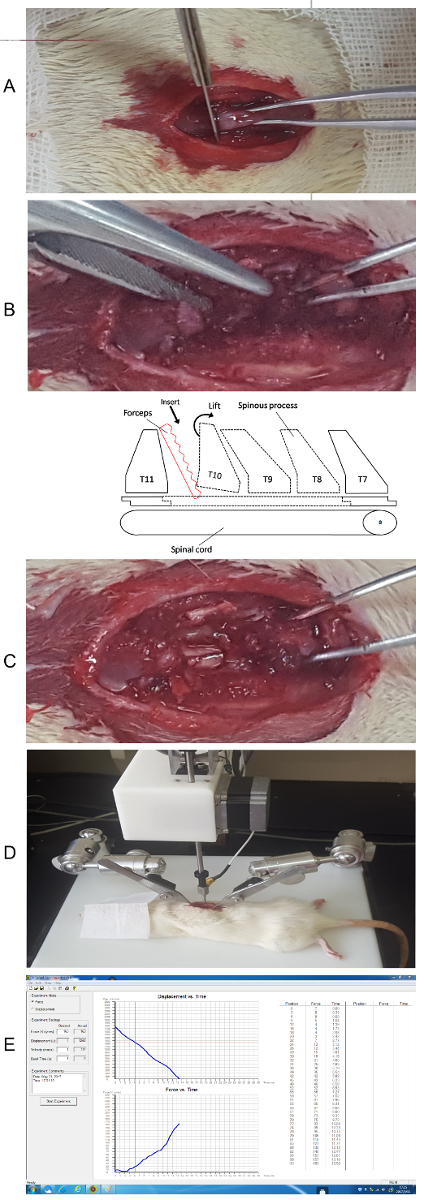
Figure 1. Laminectomy and the concussion to the spine. (A) Disconnect the junction between T10 and T11. (B) Insert the forceps to break the pedicle. (C) Break the lamina and expose the spinal cord. (schematic sketch of the anatomy) (D) Stabilize the spine on the experiment table. (E) Initial impact using the software and check the data. Please click here to view a larger version of this figure.

Figure 2. Step by step setup for laser Doppler scanning. (A) General setup for scanning. (B) Setup interface for image scan parameters. (C) Setup interface for video and distance. (D) Setup interface for repeat scan. Please click here to view a larger version of this figure.
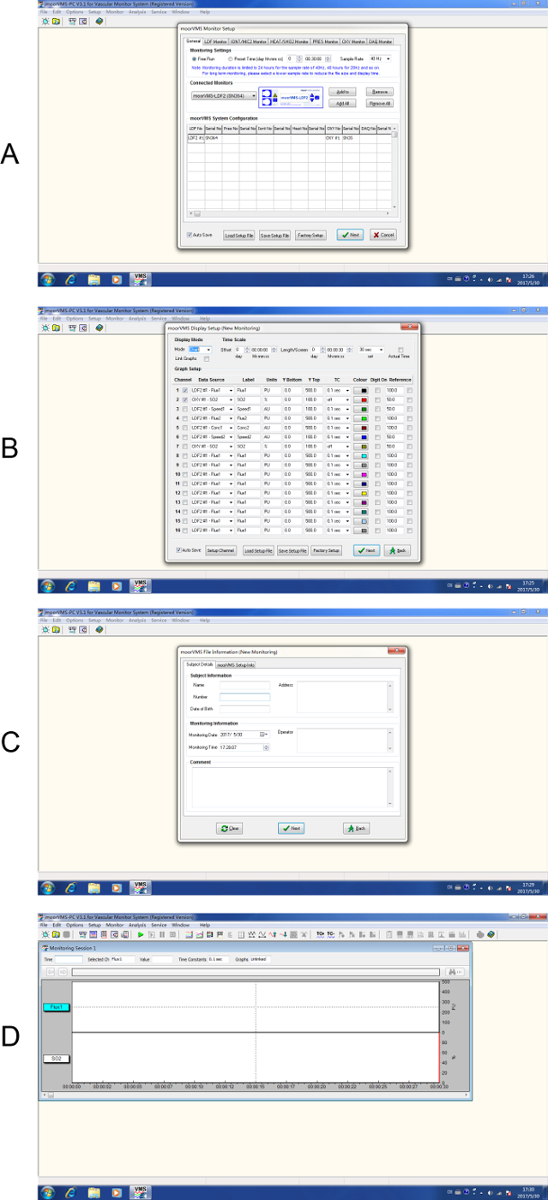
Figure 3. Step by step setup for laser Doppler monitoring. (A) Start a new experiment. (B) Select channel display. (C) Input subject details. (D) To start data recording. Please click here to view a larger version of this figure.
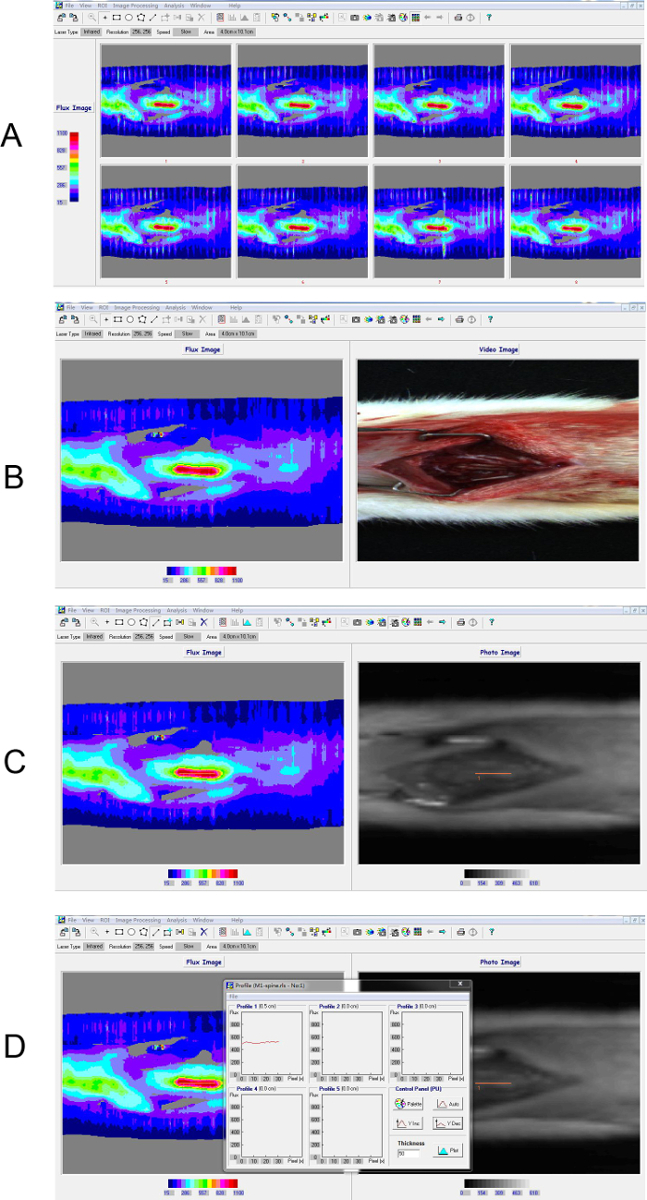
Figure 4. Process of laser Doppler perfusion imaging. (A) 8 continuous scans derived by scanning rats in the sham group. (B) The average image of the continuous scans. (C, D) Region of Interest (ROI) was selected based on the infrared image to extract the intensity profile along the central axis of the spine. The inset box shows the profiling result of the ROI. The color bar indicated perfusion units measured by laser Doppler scanner where blue represents the lowest value and red represents the highest value. The instrument detected the relative value of perfusion, namely "flux". Please click here to view a larger version of this figure.
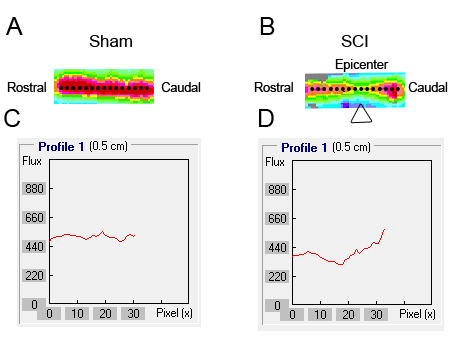
Figure 5. BF of the spinal cord was detected using laser Doppler perfusion imaging. (A, B) A 5 mm ROI was drawn on the flux map along the axis of the spine from the rostral to the caudal cord. (C, D) The intensity profile of each ROI along a line centered on the spinal cord axis was extracted for quantification.
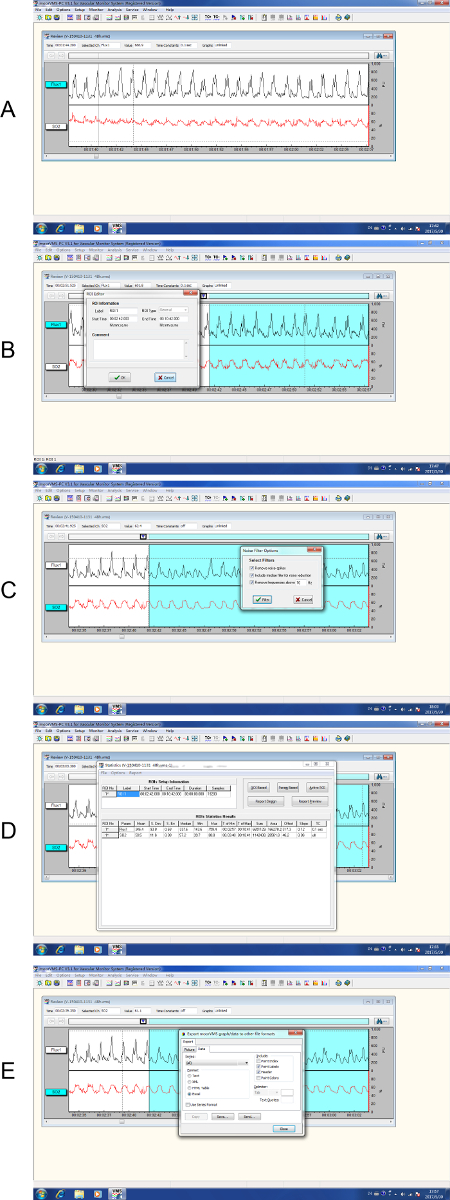
Figure 6. Process of laser Doppler perfusion monitoring. (A) The recording of raw data where the time marker indicated the starting point. (B) Selection of an 8 min ROI. (C) The selected data were then filtered by a built-in filter. (D) Statistical analysis of ROI. (E) Export of the raw data. Please click here to view a larger version of this figure.
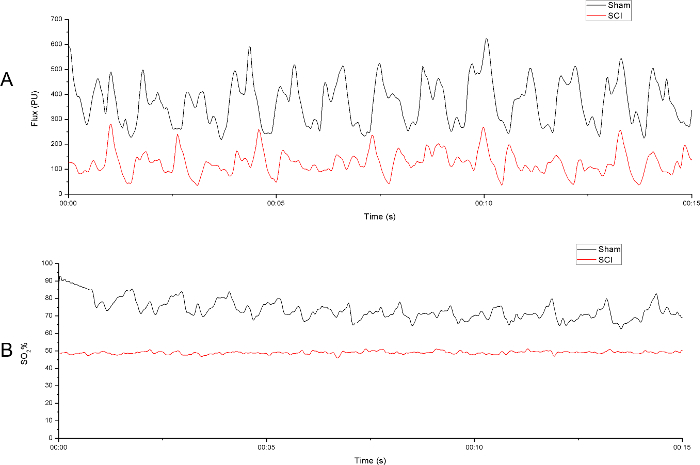
Figure 7. Spinal cord perfusion was evaluated by laser Doppler perfusion monitoring. (A) A 15 s sample of the raw blood flow output from both sham group and SCI group. (B) A 15 s sample of the raw oxygen saturation output from both sham group and SCI group. The laser Doppler probe was positioned 2 mm rostrally to the middle point at the level just above the surface of the spinal cord to the right side of the central vein. Please click here to view a larger version of this figure.
