- The implantation of a miniaturized nitinol stent into the left carotid artery of mice takes 25-30 min and shows a mortality rate of 10% mostly due to the damage of the vessel during the intervention. A better survival rate is observed in mice having a weight more than 25 g at the time of stent implantation (mortality rate of 5%). Therefore, we chose for the implantation mice with a weight between 25-27 g. After surgery, the mice recover from anesthesia within 2-5 min and no physical impairments, like e.g. paralysis, are observed. Micro-Computer Tomography (Micro-CT) imaging performed one week after stent implantation showed that the stents are not dislocated by blood flow (Figure 1C). Unfortunately, analysis of neointima formation in these images is not possible due to the metal-derived artifacts (Figure 1D, 1E).
- We didn’t observe any vessel or endothelial damages of unstented area of the vessel, immediately below the stent, as detectable by histological (Figure 2A) and by specific staining for endothelium (Figure 2B, anti-mouse CD31 antibody). For a better overview, the section was scanned using a two-photon laser scanning microscopy (Figure 2B, 2C).
- In the stented vessel, a permanent dilatation of 15% is detected (ratio stent:artery, 1,15:1) by mice with a weight between 25-27 g. Neointima formation and thrombus-formation can be analyzed by classical histological stainings (e.g. Hematoxilin-eosin, Giemsa, Movat, Toluidin Blue, Masson-Trichrom-Goldner, Figure 3A, 3B). Since the lamina externa and interna are not visible anymore, plaque size was calculated as the difference of the external and the luminal areas (mean plaque area: 234566 ± 3315 μm2, mean luminal area: 12036 ± 2662 μm2). External circumference was also measured (mean: 1799 ± 14 μm). For analysis of the cellular composition, the sections need to be deplastified and stained with specific markers. For the re-endothelialization, we used a Cy3-conjugated anti-CD31 antibody and for smooth muscle cell proliferation a FITC-conjugated anti-SMA antibody (Figure 3C). Re-endothelialization was calculated as percentage of CD-31 positive stained to the total luminal surface (mean: 23.07 ± 3.14 %) one week after stent implantation.
Of course, an unlimited number of specific staining is possible, depending on each laboratories’ experience. Analysis of myosin heavy chain, for a better characterization of SMCs, but also analysis of infiltrated cells (monocytes, lymphocytes), or stainings for different inflammatory cytokines can also be performed, depending on the aim of the study.
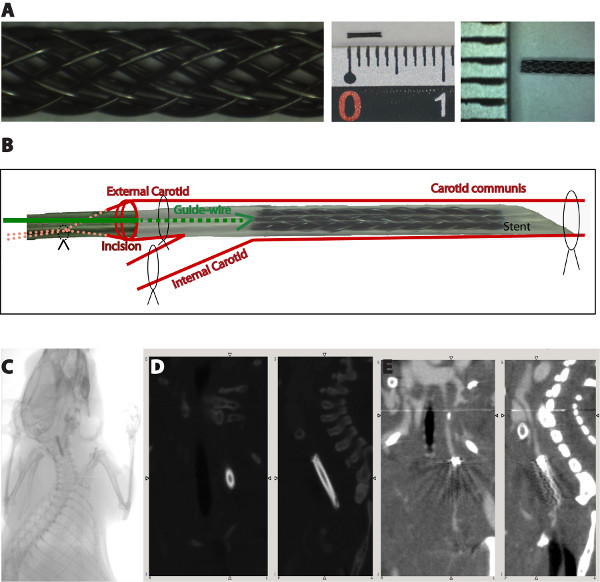
Figure 1. Schematic overview of the surgical procedure (A). The blood flow is interrupted by binding the knots on the internal carotid artery and the proximal external carotid artery firmly, as well as by pulling the knot surrounding the common carotid artery. The silicon tube containing the stent is introduced into the external carotid artery through a small incision at the external carotid artery. After the stent reaches the desired position, the silicon tube is pulled back over the guide-wire and allows the shape-memory expansion of the stent. Micro-CT images showing the stent position one week after surgical implantation (B). Due to the material-derived artifacts, an analysis of the neointima growth is not possible (C,D).
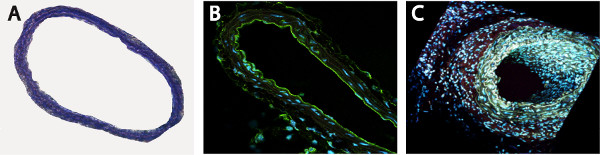
Figure 2. Unstented area of the vessel is not affected by the surgical procedure, as shown by Toluidin Blue (A) and endothelial-specific CD31 staining (B, C).
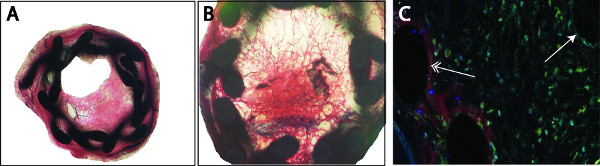
Figure 3. Analysis of the plaque can be performed by classical histological stainings (e.g. Masson-Trichrom-Goldner) (A). The organized thrombus can be detected by black-stained fibrin depositions inside the neointima, in some cases a complete occlusion of the vessel is observed (B). Re-endothelialization (Cy3, red) or smooth muscle cell proliferation (FITC, green) was detected by double immunofluorescence staining using specific markers. Counterstaining was performed with 4′,6-diamidino-2-phenylindole (DAPI, blue) (C). We noticed a completed re-endothelialization of the stent struts (left, double arrow) compared to an incompleted luminal re-endothelialization (right, single arrow).
