A total of six animals were included in the study. In all the animals, the pacing lead was successfully implanted via the external jugular vein into the right ventricular apex (Supplemental Figure S1). The position was verified by fluoroscopy, and the lead was stitched to the adjacent tissues over a rubber sleeve. According to the X-ray imaging, the lead maintained its position over the whole pacing protocol period. The attached pacemaker was palpable in the lateral neck region, causing no obvious trouble to the animal. All the wounds healed fully and without local complications.
The lead tip was equipped with two titanium-platinum electrodes — a distal hemispherical ring, and a proximal cylindrical ring electrode — with an interelectrode distance of 25 mm (Figure 2). The leads were freely advanced into the apex and passively attached there by their silicon fixing tines. This allowed for unipolar pacing from the tip electrode and for bipolar pacing between both electrodes located in the right ventricle.
A representative ventricular myocardial potential sensed signal is shown in Figure 3, and the measured pacing parameters are given in detail in Table 1 and Figure 7. At the time of the procedure, the mean sensed myocardial potential was 5.6 V ± 0.8 mV (min: 2.8 mV, max: 8 mV), the lead impedance was 675 Ω ± 74 Ω (min: 468 Ω, max: 951 Ω), and the pacing threshold was 0.8 V ± 0.26 V (min: 0.2 V, max: 2.2 V), with the stimulus duration set to the standard 0.4 ms.
After follow-up of 3 months and 6 months with intermittent pacing, the mean sensed myocardial potential was 7.4 mV ± 1.2 mV (min: 4.0 mV, max: 12.0 mV) and 6.3 mV ± 1.0 mV (min: 4.2 mV, max: 10.3 mV), respectively. The mean lead impedance measured was 869 Ω ± 32 Ω (min: 760 Ω, max: 975 Ω) and 725 Ω ± 96 Ω (min: 370 Ω, max: 1014 Ω), respectively, and the pacing threshold changed to 1.2 V ± 0.3 V (min: 0.2 V, max: 2.2 V) and to 1.4 V ± 0.3 V (min: 0.5 V, max: 2.3 V), respectively. All the parameter changes were not statistically significant over this period (P > 0.05), and the bipolar and unipolar parameters followed comparable trends (Figure 7 and Table 1).
One case was terminated early due to partial lead penetration, which presented with an abrupt impedance drop observed on the second day after the implantation. Later, during the second month of follow-up, a gradual threshold increase was noticed, and pacing on high output caused muscular fasciculation. The animal remained asymptomatic, but during necropsy, the tip of the pacing lead was found to have penetrated through the myocardial inferior wall into the pericardium by a length of approximately 3 mm. No bleeding and no signs of infection were observed.
Before the procedure, on day 1 post procedure, and on day 7 post procedure, the mean white blood cell counts were 5.9 × 109/L, 7.37 × 109/L, and 7.42 × 109/L, respectively, the mean hemoglobin levels were 105 g/L, 113 g/L, and 110 g/L, respectively, and the mean platelet counts were 317 × 109/L, 274 × 109/L, and 219 × 109/L, respectively. The laboratory values did not demonstrate significant changes during the first week after the procedure (P > 0.05 for all). Under microscopic evaluation, the pacing lead silicon surface was covered by fibrous tissue (with an approximate thickness of 100 µm), but no cells were found (Figure 8).
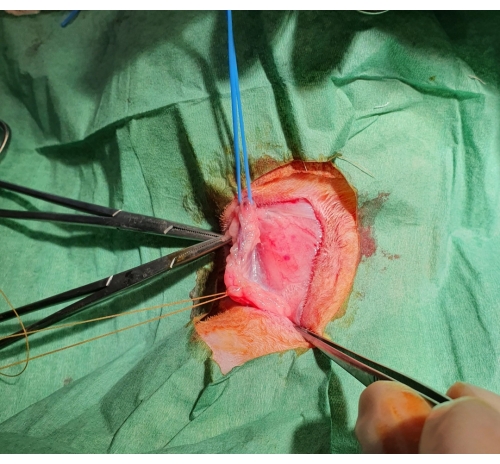
Figure 1: Surgical jugular vein dissection. After the skin is cut, a subcutaneous pocket is formed, and the jugular vein is exposed, ligated distally, and supported by a blue rubber band proximally. Please click here to view a larger version of this figure.
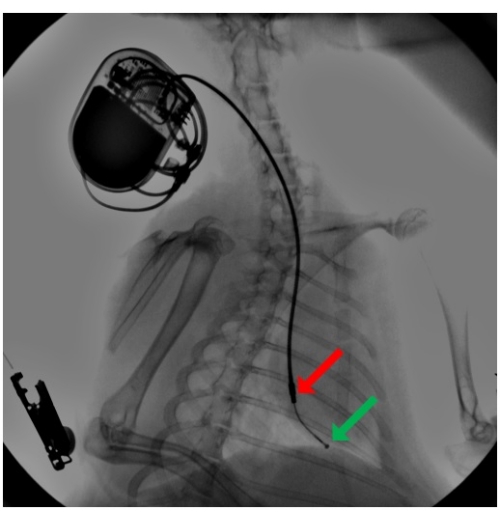
Figure 2: Fluoroscopy during pacemaker lead implantation. A pacing lead is introduced via the external jugular vein, and using a pre-shaped stylet, the lead advanced to the right ventricular apex, where it is secured by passive fixation by its silicon tines. An attached pacemaker is buried in a subcutaneous pocket in the neck region. The arrow point to the distal hemispherical ring (green) and the proximal cylindrical ring (red) electrodes. Please click here to view a larger version of this figure.
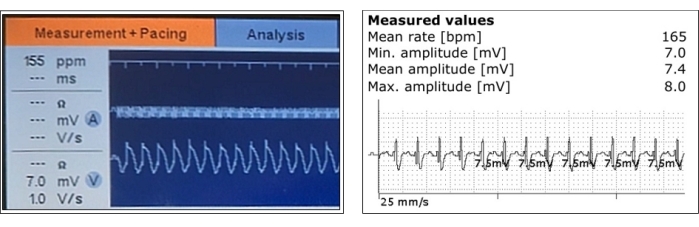
Figure 3: Representative measurements of sensed ventricular myocardial potentials. Ventricular sensing and its amplitude measurements are shown during the acute phase after pacing lead positioning (left) and after the pacemaker implantation (right). Please click here to view a larger version of this figure.
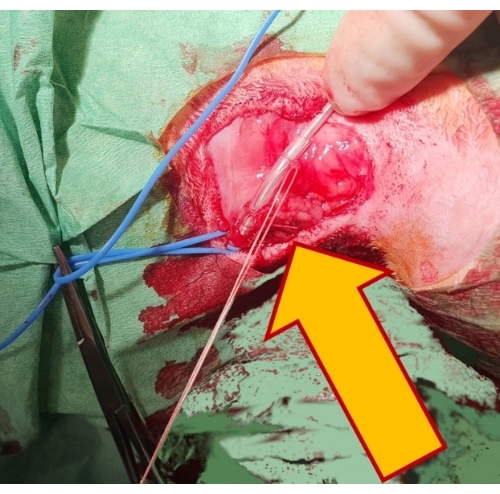
Figure 4: Securing the pacing lead. Fixing the lead by two non-absorbable sutures over a rubber sleeve (arrow) to the underlying tissue secures it in position and prevents its dislocation. Please click here to view a larger version of this figure.
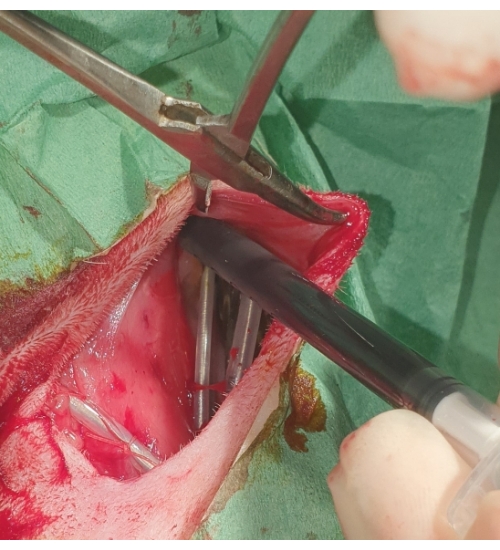
Figure 5: Placement of the pacemaker. The pacemaker is buried into the subcutaneous pocket and flushed with povidone-iodine. Please click here to view a larger version of this figure.
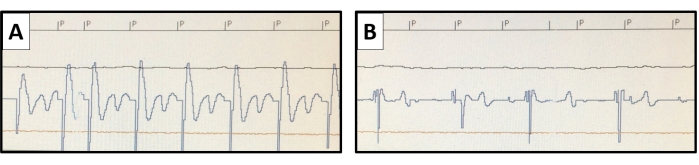
Figure 6: Pacing threshold measurement. Using the non-invasive pacing study function of the pacemaker, pacing at higher than the native heart rate is conducted. The pacing stimuli are marked with P. The pacing threshold is evaluated with varying stimulus outputs. (A) A representative example of the endocardial potential of ventricular capture is shown for an output of 0.8 V at 0.4 ms, (B) but a loss of capture is seen with the output reduced to 0.6 V at 0.4 ms. Please click here to view a larger version of this figure.
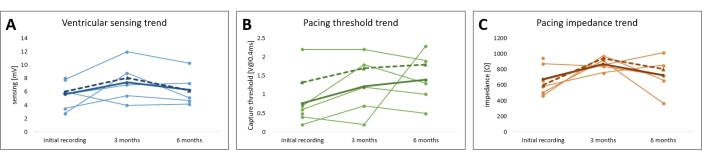
Figure 7: Follow-up of the leporine cardiac pacing model pacing parameters. The trends of the (A) pacing threshold, (B) pacing impedance, and (C) myocardial sensing for all the subjects are plotted. The average unipolar (full line) and bipolar values (dotted line) are shown in bold. Please click here to view a larger version of this figure.
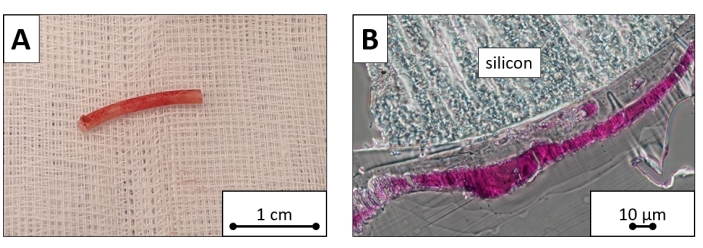
Figure 8: Explanted pacing lead sample. Ventricular portion cut of the explanted pacing lead. (A) The macroscopic image and (B) microscopic image dyed with toluidine blue reveal the silicon surface covered by a layer of fibrous tissue. Scale bars = (A )1 cm, (B) 10 µm. Please click here to view a larger version of this figure.
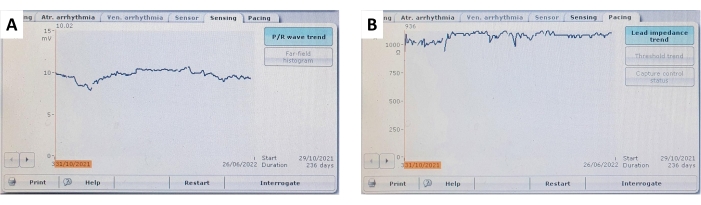
Figure 9: Ventricular sensing and lead impedance trends. A representative example of (A) continuous and stable ventricular myocardial sensing and (B) ventricular lead impedance trends over a follow-up of 236 days. Please click here to view a larger version of this figure.
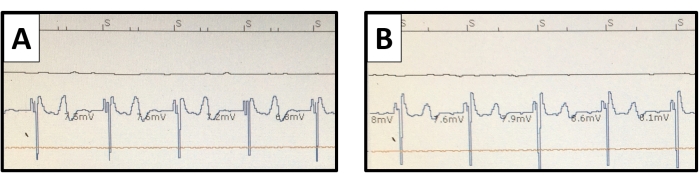
Figure 10: Ventricular endomyocardial electrograms. The pacemaker interrogation sensed ventricular potentials are pictured with (A) unipolar and (B) bipolar connections. The T wave potential is more distinct with the unipolar connection but does not cause oversensing. Please click here to view a larger version of this figure.
| Unipolar | periprocedural | follow-up | |||||||
| 3 months | 6 months | ||||||||
| Sensed myocardial potential [mV] | 5.6 ± 0.8 | 7.4 ± 1.2 | 6.3 ± 1.0 | ||||||
| Pacing threshold [V at 0.4 ms] | 0.8 ± 0.3 | 1.2 ± 0.3 | 1.4 ± 0.3 | ||||||
| Lead impedance [Ω] | 675 ± 74 | 869 ± 32 | 725 ± 96 | ||||||
Table 1: Follow-up of the leporine cardiac pacing model pacing parameters. The values of the sensed myocardial potential, pacing threshold, and lead impedance are expressed as mean ± SEM for 3 months and 6 months of follow-up.
Supplemental Figure S1: Schematic of the implanted human-sized transvenous pacing system in a rabbit. Please click here to download this File.
