Measuring the movement of the small foot bones is critical for understanding pathological loss of function. However, dynamic foot bone motion measurement is challenging due to the small size and densely packed configuration of the bones and joints1,2. Biplanar videoradiography (BVR) technology is well-suited to measure the in vivo three-dimensional (3D) motion of the small bones of the foot and ankle during dynamic activities. BVR provides insights into arthro-kinematics by using two x-ray sources coupled to image intensifiers, which convert x-rays of dynamic motion to visible light. As the foot moves through the capture volume, high-speed cameras capture the images. The images are un-distorted and projected into the capture volume using calibrated camera positions3,4. The six degrees of freedom (6 d. o. f.) bone pose (3 d.o.f. for position and 3 d.o.f. for orientation) is then estimated using either marker-based or model-based methods3.
The marker- or model-based pose estimation methods vary among laboratories and disciplines. The gold standard of dynamic BVR pose measurement is the implantation of small tantalum markers into the bone of interest4,5. A minimum of three markers per bone is required to estimate the pose, with additional markers leading to higher accuracy5,6. This method is less common in vivo due to its invasiveness, as it requires surgical implantation, and the markers are then embedded permanently in the bone7. Alternatively, model-based tracking uses volumetric information from other imaging modalities, such as computed tomography (CT) or magnetic resonance imaging, to recreate the model on the BVR images2,3,8,9,10,11,12,13,14,15. The model is then semi-manually manipulated to best match the images (rotoscoping), typically using a combination of user input as an initial estimation and cross-correlative optimization3,8,9,10,15. Model-based pose estimation is less invasive, and therefore more common, but has a greater processing time and requires user input. As the rotoscoping process is currently semi-manual, there remains a need to reliably train operators in the lab-specific software as inter-operator root mean square (RMS) errors can range from 0.83 mm to 4.96 mm, and 0.58° to 10.29° along or about a single axis1. Further, model-matching algorithms are improving, but require validation using experimental paradigms that are as close to in vivo conditions as possible.
The accuracy of model-based pose estimations is often assessed against marker-based metrics. For example, human cadaveric feet implanted with markers have been moved through simulated locomotory positions13,14,16. The captured BVR images are then fed to the model-based rotoscoping method and compared to the marker-based metrics for accuracy (bias and precision). While the use of a static cadaver foot is a valuable approach, it has limitations in assessing true in vivo bone pose accuracy. For example, joint positions are relatively constant in a cadaver foot with the absence of muscular activity and in vivo loads. Thus, it may not represent the limits of joint motion in diverse locomotor tasks. Variations in joint posture change the occlusion in the BVR images, which is a source of measurement error when estimating small, densely packed foot bone poses13. Further, when using image-matching algorithms, the presence of markers in the BVR images would likely bias the results. While groups have removed the markers from the computed tomography (CT) digital imaging and communications in medicine (DICOM) images9,14,16, they are only occasionally also removed from the biplanar videoradiography images16.
This work presents an open-source BVR dataset of a participant hopping and running in vivo, who has markers implanted in his foot and ankle bones (Figure 1). Marker-based pose estimation for the in vivo bone motion of the tibia, talus, and calcaneus is provided. The markers were removed from both the x-ray and CT images to limit any bias introduced during the assessment of model-based tracking accuracy. This dataset is intended for assessing the accuracy of any model-based pose estimation software, and for improving the selection of initial pose estimates for semi-manual processes. It is most appropriate for individuals who aim to improve the speed and accuracy of the BVR image processing pipeline, and for laboratories that desire low inter-operator variability in initial pose estimation.
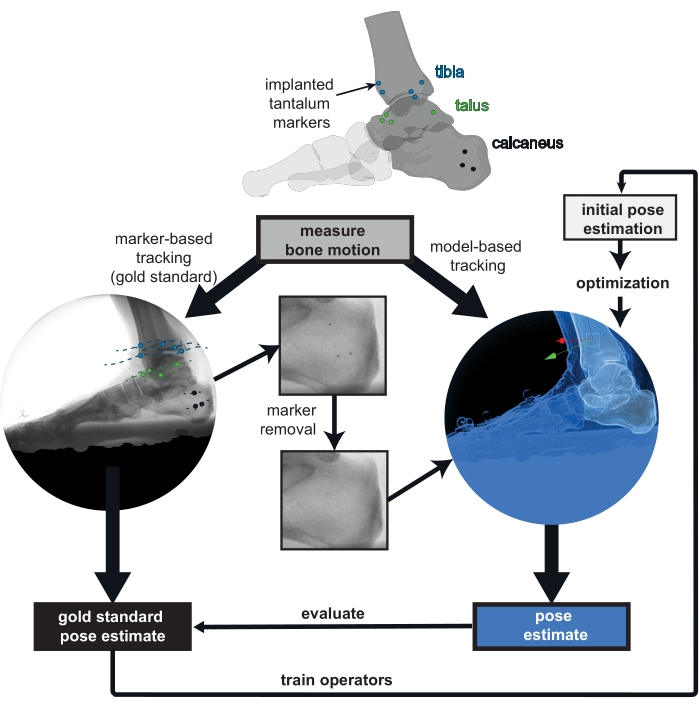
Figure 1: Overview of the provided biplanar videoradiography (BVR) dataset. Implanted markers are tracked in vivo as the gold standard for bone pose estimation. The markers were digitally removed from the BVR images and the computed tomography scans to prevent bias in the model-based tracking. Poses estimated from any model-based tracking software can be compared to the gold standard of marker-based tracking. The marker-based pose estimate can also be used to train new operators to improve their initial bone pose estimation for model-based tracking. Please click here to view a larger version of this figure.
Experimental protocols were approved by Queen's University Health Sciences and Affiliated Teaching Hospitals Research Ethics Board. The participant gave informed consent prior to participation in the data collection.
1. Patient preparation and dataset generation
NOTE: The participant (male, 49 years, 83 kg, 1.75 m tall) had several 0.8 mm diameter tantalum markers previously implanted into the calcaneus (3 markers), talus (4 markers), and tibia (5 markers; Figure 1).
- Acquire a CT scan with a metal artifact reduction algorithm (to reduce the image distortion due to metal implants) on the participant's foot in a maximally plantarflexed ankle posture with a pixel size of 0.500 mm or less, and a slice thickness of 0.625 mm or less.
NOTE: Here, the participant's right foot was scanned at a resolution of 0.441 mm x 0.441 mm x 0.625 mm. The markers' locations are not placed at specific anatomical locations within the bone4; instead, they are distributed throughout the bone5. - For methods for collecting biplanar videoradiography and processing the data in detail, see17. Briefly, ask the participant to complete the desired movement, with their start position curated such that their foot lands in the biplanar videoradiography volume. Use a calibration object and un-distortion grids to locate the cameras and un-distort the images, respectively18.
NOTE: The participant in this study completed trials of two different movements. They hopped to a metronome at 108 bpm and jogged slowly through the volume. Images were captured continuously at 250 Hz with a 1111 µs shutter speed, and the x-ray system was set to 70 kV and 100 mA. - Individually segment the markers using 3D medical image processing software. Using the content-aware fill algorithm in the raster graphics editor and the known marker locations, remove the markers from the DICOM images. Create the bone partial volumes and tessellated meshes by segmentation of the marker-less images as shown in17. Align both the partial volumes and the meshes and store them in CT space.
- For each frame, tabulate the unfiltered x-y image coordinates of each marker in XMALab and export it18. Triangulate the 3D coordinates using the computer vision toolbox in MATLAB. Estimate the pose by matching the 3D marker positions in x-ray space to the sphere-fit centroids in CT space using a least-squares approach19. Use the same algorithm in the raster graphics editor to remove the markers in the x-ray images to prepare them for tracking.
2. Access the dataset and code
- Download the dataset from burada. There are BVR images and calibration files for each trial, as well as reference pose estimates saved in the .tra format (Figure 2). Download/clone the code package from: https://github.com/skelobslab/JOVE_BVR_FootModelAndMarkerBased.
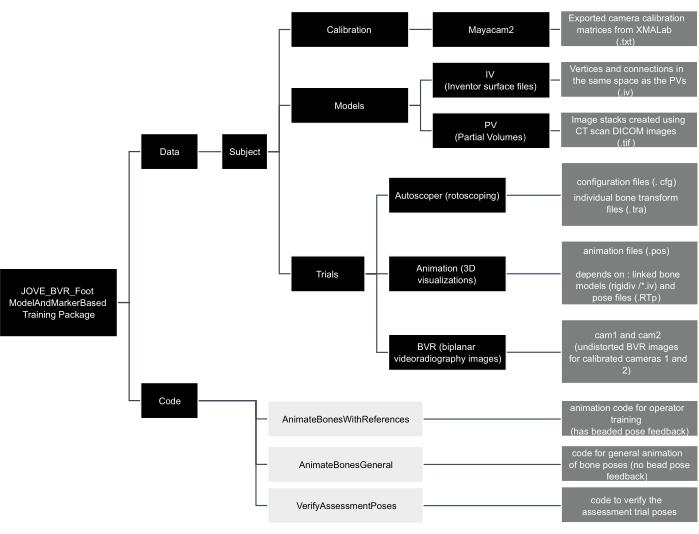
Figure 2: Data tree of the JOVE_BVR_Foot_ModelAndMarkerBased training package. Folders are shown in black boxes, code is shown in light grey boxes, and descriptions of files are contained in dark grey boxes. Please click here to view a larger version of this figure.
3. Assess the accuracy of the model-tracking algorithm
- Save pose estimates as a .tra file in the trial's reference folder. Arrange the .tra file with the pose from bone space to x-ray space written in a 1-row x 16-column format, with each row corresponding to the frame and the 4 x 4 pose matrix written out as [first column, second column, third column, and fourth column].
NOTE: Bone space is synonymous with CT space in this dataset. - Verify pose estimates by opening the script verifyAssessmentPoses.m in the computing platform and then clicking Run. Load the files as described by the prompts. The script will calculate the helical axis between the model- and marker-based pose estimate and return a rotation and translation difference for each frame of tracked data.
4. New operator training
NOTE: This section describes the training with feedback for a new operator. Here, Autoscoper is the selected model-based pose estimation software, but other software could be used as a replacement.
- Download the latest version of the pose estimation software from: https://simtk.org/projects/autoscoper.
- To locate local BVR files, open the file in a text-editor (.JOVE_BVR_Foot_ModelAndMarkerBasedDataSOL001AT0019_jog0001AutoscoperPOINTER_T0019_jog001.cfg). The software uses a pointer file (.cfg) to locate files. Modify the directories so that they lead to the appropriate local files. Save the file and close it.
- To load the BVR images and camera information, open the pose estimation software and click Load Trial. Navigate to the pointer configuration file saved in the previous step and click Open.
- To track, follow the protocol in Akhbari et al17 (model-based tracking). In brief, rotate and translate the bone by clicking and dragging the axes on the bone until satisfied with the position and orientation of the calcaneus. Press the S key on the keyboard to save the current frame for the calcaneus (cal).
NOTE: Filter settings are included in JOVE_BVR_Foot_ModelAndMarkerBasedDataSOL001AT0019_jog0001Autoscoper which can be used for filtering as shown in Akhbari et al17. - To save the files, click Save Tracking. Save the file as [Trial number]_[Subject Number]_[Trial name]_[3 letter bone code].tra (e.g., T0019_SOL001A_jog0001_cal.tra) under the desired directory. Export the settings as current, matrix, column, comma, none, mm, degrees.
NOTE: The three-letter bone codes for the tibia and talus are tib and tal, respectively. - To create files for tracking accuracy, open the computing platform and run the animateBonesWithReferences.m script in the code folder. Navigate to the folders within the training package as requested by the dialog boxes.
NOTE: The animateBonesWithReferences.m code is a specialized code for training that provides the poses from marker-based data as feedback to improve the new operator's tracking. - Install visualization software from: https://github.com/DavidLaidlaw/WristVisualizer/tree/master. To visualize the tracking, open the .pos file created in step 4.6 in the visualization software; its file location will be in the computing platform’s command window.
- Verify the alignment of the tracked bone (grey) with the reference bone. Green color indicates the pose is within the rotation and translation thresholds while red indicates it is outside the threshold. Continue tracking and visualizing until all frames are green. Change the thresholds (phi – rotation, trans – translation) in lines 10 and 11 of the animateBonesWithReferences.m script, if required.
NOTE: If the reference bone is red (Figure 3A), it means the pose is more than 1 mm or 2° away from the marker-based pose, as measured using the helical axis. If it is green, and visually is reasonable, that frame is tracked sufficiently well (Figure 3B). - To track the other bones in the ankle complex, repeat steps 4.4 to 4.8 for the talus and tibia. Use the visualization software to ensure that the bones are not colliding.
- To complete the assessment, track and visualize the tibia, talus, and calcaneus in the trial called assessment trial.
- Open the computing platform and run the code animateBonesGeneral.m. Navigate to the folders within the training package as requested by the dialog boxes. Verify the bone poses using the .pos file in the visualization software. This code is generalizable to other trials for 3D visualization of the bones.
NOTE: The true, marker-based pose will no longer be available. Only the grey bones will be present.
- Open the computing platform and run the code animateBonesGeneral.m. Navigate to the folders within the training package as requested by the dialog boxes. Verify the bone poses using the .pos file in the visualization software. This code is generalizable to other trials for 3D visualization of the bones.
- To evaluate the pose estimates, open the script verifyAssessmentPoses.m in the computing platform and click Run. The script will calculate the helical axis between the model- and marker-based pose estimate and return a rotation and translation difference for each frame of tracked data. This will produce the same graph as in animateBoneswithReferences.m but will not produce an animation.
- Verify that all data points are below the selected threshold (flat line) for both rotation and translation. Save the results out in a .csv file, if required.
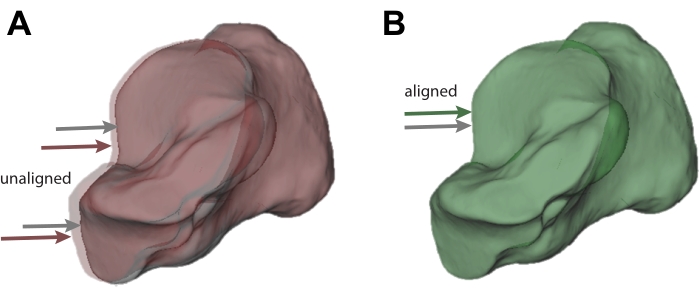
Figure 3: Visualization of acceptable and unacceptable tracking. (A) Calcaneus bone tracked using model-based tracking (grey; also indicated by the grey arrow) that does not sufficiently match the pose from the marker-based pose estimate (red; also indicated by the red arrow). (B) Calcaneus that sufficiently matches the pose from the marker-based pose estimate. The marker-tracked calcaneus is shown in green as a result (also indicated by the grey and green arrows). Please click here to view a larger version of this figure.
Two new operators and one expert completed the model-based training. The 41 frames of the assessment trial measured the proficiency of their model-based tracking (Figure 4). The operators' pose estimates were typically well below the set thresholds. The mean median bias (range) in rotation across bones was 0.75° (0.69° to 0.85°) for the calcaneus, 0.40° (0.37° to 0.46°) for the talus, and 0.89° (0.76° to 1.07°) for the tibia. The mean median translation bias was 0.10 mm (0.05 mm to 0.16 mm) for the calcaneus, 0.31 mm (0.22 mm to 0.41 mm) for the talus, and 0.33 mm (0.27 mm to 0.37 mm) for the tibia. These results suggest that the tutorial is effective at training the operators to within a set tolerance.
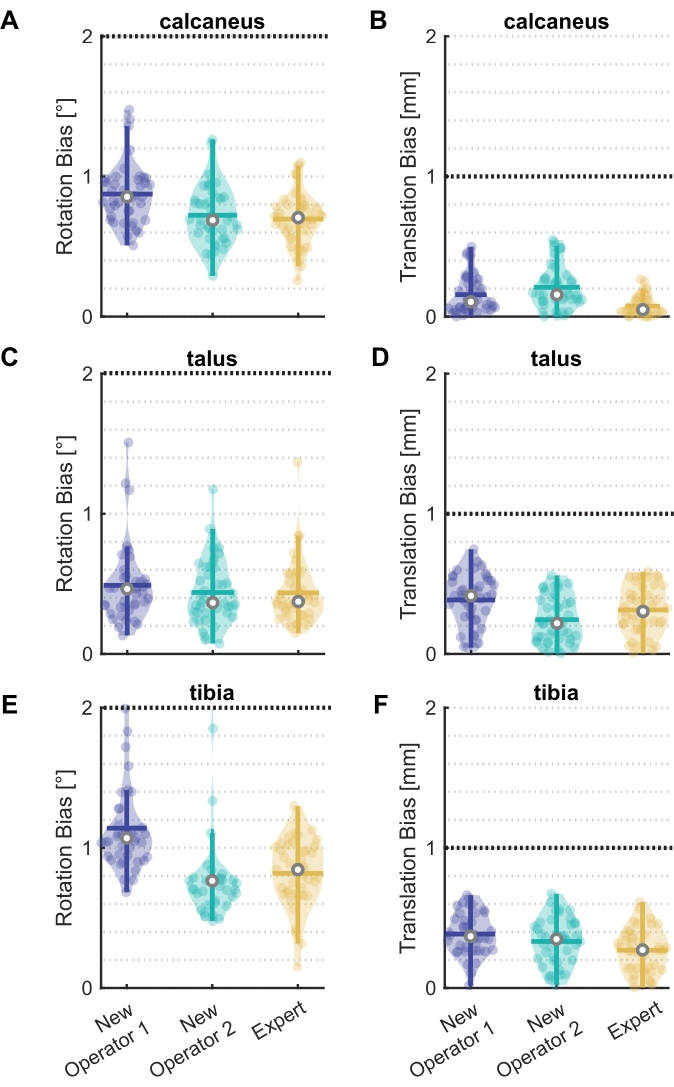
Figure 4: Rotation and translation bias for new operators and an expert. Violin plots20 showing bias in (A)(C)(E) rotation and (B)(D)(F) translation between model-based and marker-based pose estimates for two new operators and one expert for the (A)(B) calcaneus, (C)(D) talus, and (E)(F) tibia. All 41 frames of the assessment trial are shown as data points, with the median (white circle), interquartile range (thick vertical line), and mean (thick horizontal line). The black line at 2° and 1 mm represent the selected thresholds. Six frames outside the threshold for New Operator 2 in (E) are not shown. Please click here to view a larger version of this figure.
One new operator had six frames above the 2° rotation threshold in their tibia tracking. The frames were identified using one of the generated graphs in verifyAssessmentPoses.m (Figure 5). These six frames are more difficult to track due to tibia occlusion by the other foot swinging through the view.
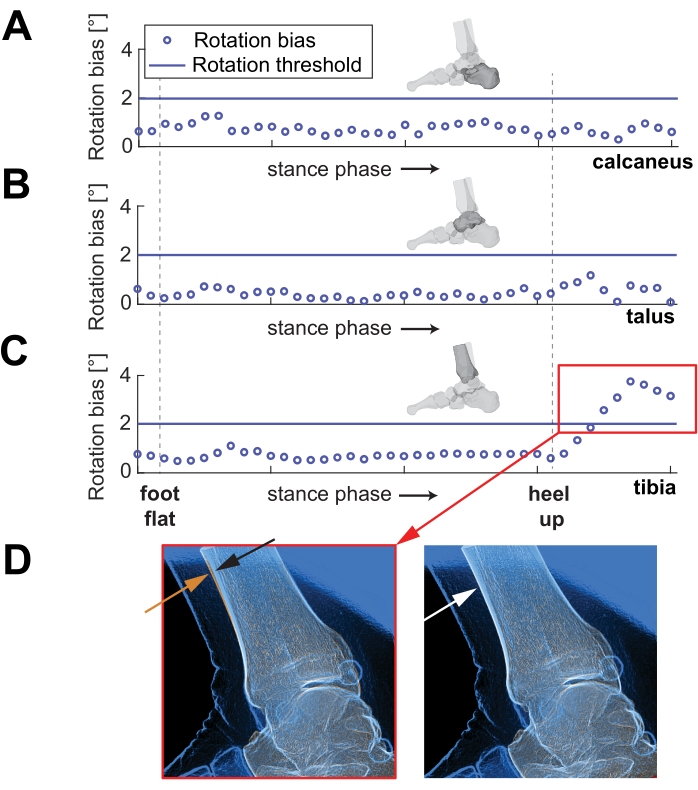
Figure 5: Rotation bias for each frame over stance phase. Example of the second new operator's rotation tracking over part of stance phase of running, for (A) the calcaneus, (B) the talus, and (C) the tibia. Note the red box in (C) shows the frames with high errors. (D) On the left, a representative image shows the approximate difference in alignment of the orange and blue lines of the anterior tibia (indicated by orange and black arrows). The right image shows an example of a well-tracked tibia (indicated by the white arrow). Please click here to view a larger version of this figure.
Supplemental File. Please click here to download this File.
