Perfusate Preparation
Upon successful employment of the in-bore oxygenation device, gases present in the supplied carbogen will reach 100% saturation conditions within the aCSF perfusate. This can be demonstrated by varying the oxygen concentration of the supplied gas and measuring the change in dissolved oxygen content in the aCSF perfusate within the perfusion chamber using an oxygen meter (Figure 1)8. According to Henry's law, the amount of dissolved gas that is in equilibrium with a liquid sample is directly proportional to the partial pressure of that gas provided that the temperature remains constant12. Using this knowledge and precision gas standards, it is possible to quantify the amount of dissolved oxygen contained within an aCSF sample as described. This is achieved by calibrating the oxygen meter using saturated solutions (directly bubbled for 1 h or more) of aCSF being exposed to gasses of known composition: one gas with high oxygen concentration such as carbogen (95% O2) and another with low oxygen concentration such as nitrogen (0% O2). Afterward, measurements can be taken by submerging the tip of the oxygen electrode into a sample. Confirmation that the in-bore oxygenator is functioning properly can be achieved by measuring the effluent from the perfusion well. The percent dissolved oxygen as measured by the oxygen meter should match the percent concentration of oxygen delivered in the supply gas. If the measured values are lower than those in the supply gas, this would suggest a hardware failure that could lead to metabolic insufficiency in the tissue slice.
Sample Appearance and Behavior
Acute slice preparations that receive perfusion sufficient enough to supply necessary metabolites and carry away metabolic wastes soon reach a state of relative stability. From that point, acute slices can be subjected to external perturbation and their responses to these changes can be measured for scientific study. For MR experiments, tracking the signal of interest over time is a commonly used practice to demonstrate the relative stability of acute slice preparations13. The diffusion-weighted signal is especially sensitive to changes in a tissue's water mobility, content, and distribution, as can be appreciated by the use of this contrast mechanism to detect infarcts in ischemic stroke14,15. Plotting the normalized diffusion signal over time in acute cortical slices maintained under a variety of perfusion conditions demonstrates relatively stability (2 ± 3% over 15.5 h) after tissue isolation is achieved (Figure 5). Diffusion signal stability was maintained regardless of perfusion conditions (intermittent or continuous) or MRI scan length (short [4 min] or long [1.5 h])8. If slices do not exhibit signal stability over time, such as the sharp diffusion signal increase observed in living cortex that did not receive perfusion, this is suggestive of suboptimal experimental conditions. Perturbation experiments should not be attempted prior to confirmation of stable signal conditions in slice preparations.
In addition to signal stability, correct sample positioning must be confirmed at the time of image collection. Even though sample position is controlled during tissue placement at the dissecting microscope, shifts in sample position may occur during the assembly of the perfusion apparatus, or due to rough handling of the coil or probe prior to insertion into the magnet. Confirmation of proper hippocampal placement can be achieved by collecting short (2 min), pilot scans with diffusion contrast (Figure 6). Because the pyramidal cell layer is more sensitive to diffusion weighting than the adjacent hippocampal laminae, this structure will appear as a darker band in diffusion-weighted images. Setups that do not display this characteristic feature contain off-center samples and will likely need to be repeated.
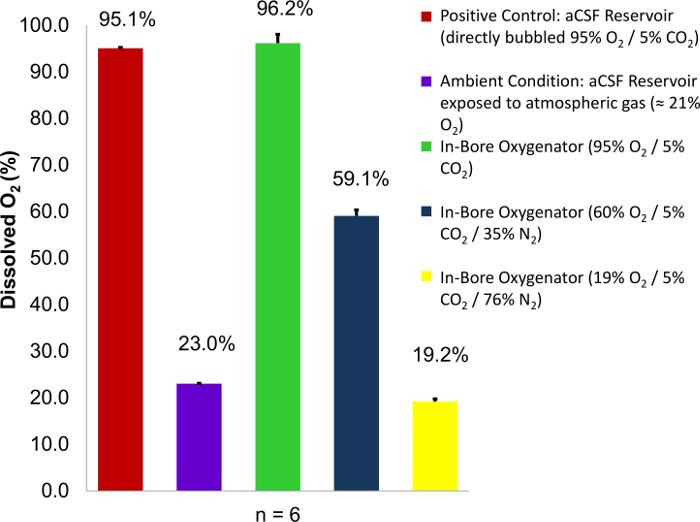
Figure 1: Dissolved oxygen content of aCSF perfusate as a function of percent O2 content in supplied gas. Carbogen mixtures containing variable concentrations of oxygen (95%, 60%, and 19%) are employed as a supply gas. Percent dissolved oxygen readings are then taken from the perfusion well and compared to two known controls: a perfusate reservoir directly bubbled with carbogen (95% O2), and a perfusate reservoir exposed to atmospheric conditions (23% O2). In each case, the percent oxygen saturation at the site of tissue perfusion approaches 100% of the O2 concentration within the carbogen mixture used. Error bars are equal to the standard deviation of the sample means. Figure reproduced with permission from the original article8. Please click here to view a larger version of this figure.
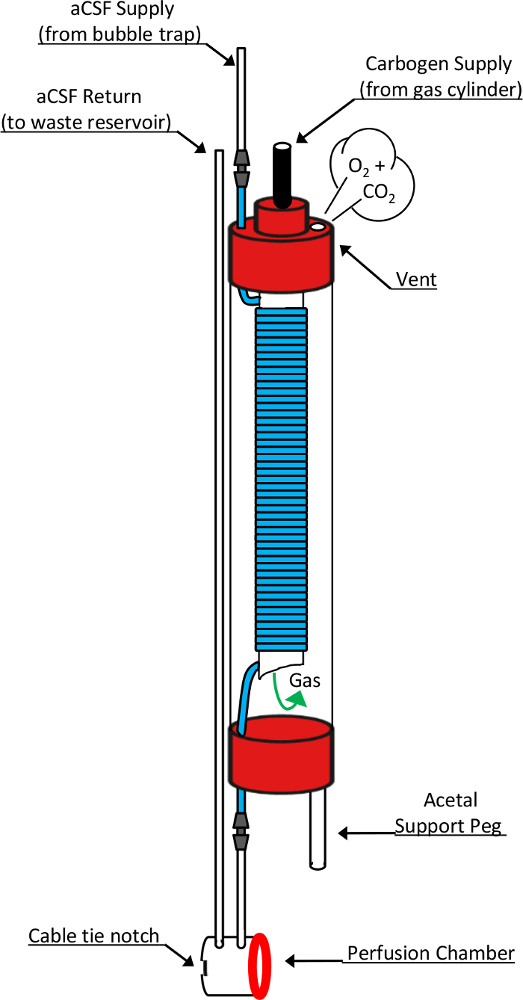
Figure 2: Schematic drawing of the in-bore oxygenator and perfusion chamber. This diagram shows detailed design elements responsible for the function of these critical devices. Fresh perfusate that has been pumped through a bubble trap enters the oxygenator through the top of a 10 mm NMR tube. In doing so, it transitions into a highly gas permeable silicone tubing (blue segment) that is coiled around an open-ended, 5 mm NMR tube nested inside. Carbogen gas supplied through the top of the 5mm tube enters the chamber through the open-ended bottom and passes over the coiled silicone tubing before exiting the oxygenator through a vent hole in the 10 mm tube cap. During this exposure, the perfusate flowing through the silicone tube becomes saturated with the chemical components of the supplied gas mixture. Upon exiting the oxygenator, perfusate passes directly into the perfusion chamber before entering the return line leading to a waste collection reservoir. Other components critical to this design include the acetal support peg which allows the oxygenator to stand vertically atop the modified RF microcoil, a silicone washer (red ring) which forms the liquid-tight seal between the oxygenator's perfusion chamber and the microcoil's tissue well, and the cable tie notch which accommodates placement of a cable tie used to form this reversible seal. This figure has been modified and reproduced with permission from the original article8. Please click here to view a larger version of this figure.
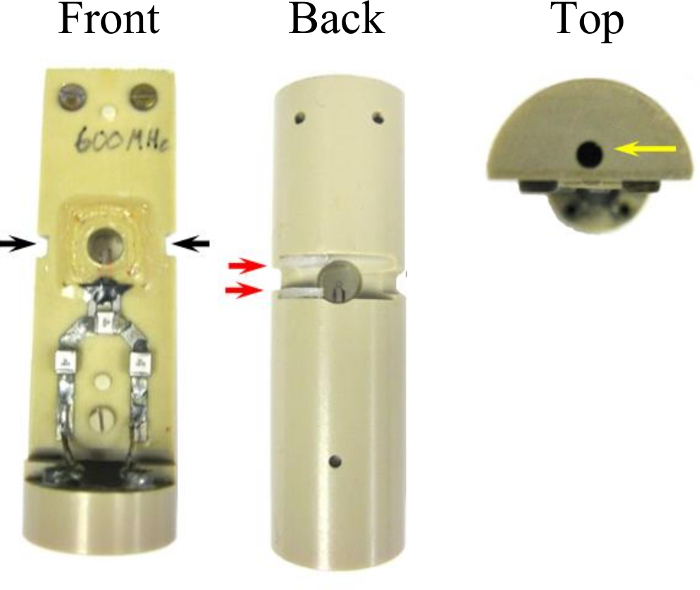
Figure 3: Modifications to the microcoil assembly which permit interface to the in-bore oxygenator. Two grooves 3.0 mm x 1.5 mm (black arrows) were cut into the side of the assembly that accommodate the width of a cable tie used to seal the perfusion chamber. A channel (15 mm x 3 mm x 4 mm) connects the groves across the back face of the coil. Two nylon spaces placed in the sides of the channel (red arrows) act as a catch for the cable tie head which eases the sealing procedure. A hole (2 mm x 14 mm) drilled in the top of the coil assembly (yellow arrow) joins to the acetal support peg to secure the oxygenator. This figure has been modified and reproduced with permission from the original article8. Please click here to view a larger version of this figure.
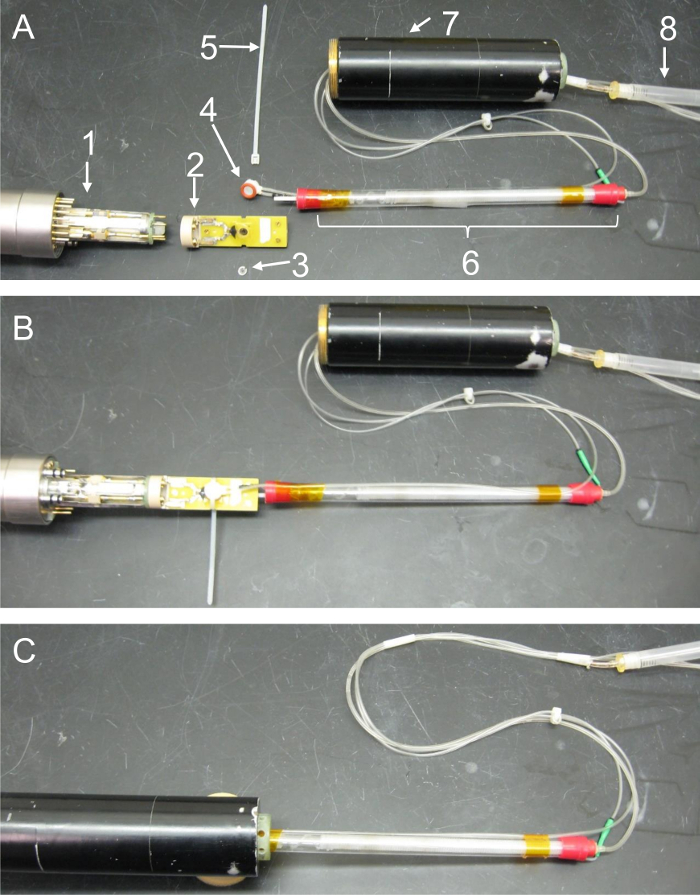
Figure 4: Photo montage detailing the relative placement and proper assembly of microcoil, oxygenator, and probe components. These images feature key hardware components of the in-bore oxygenator and microperfusion device and illustrate how the separate parts interface with one another. (A) Exploded-view photo showing the relative placement of all components prior to sealing of the tissue well or assembly of the probe body. Care has been taken to display the relative location of parts accurately; however, a section of the perfusion lines has been doubled back in this series so that all components fit within the image frame. (1 = probe head, 2 = microcoil assembly, 3 = nylon tissue retention ring, 4 = perfusion well, 5 = cable tie, 6 = in-bore oxygenator, 7 = gradient coils, 8 = bubble trap). (B) Components following coil and oxygenator assembly. In this image, the nylon retention ring has been placed within the microcoil's tissue well to secure a sample. The acetal support peg on the base of the oxygenator has been secured in the corresponding hole on top of the microcoil. The silicone gasket on the open end of the perfusion well has been placed over the tissue well, and a cable tie has been tightened around these components to seal the perfusion chamber. Lastly, the base of the microcoil has been connected to the top of the probe head. (C) Components following probe assembly. In the last panel, excess length from the cable tie has been trimmed flush with the microcoil. The gradient coil stack is then slid into position by carefully advancing the cylinder towards the probe while passing the excess perfusion lines, oxygenator, and microcoil through its hollow center. Once the gradients are connected to the probe head, they're held in place by screwing the securing collar on the probe over the threaded base of the gradients. Please click here to view a larger version of this figure.
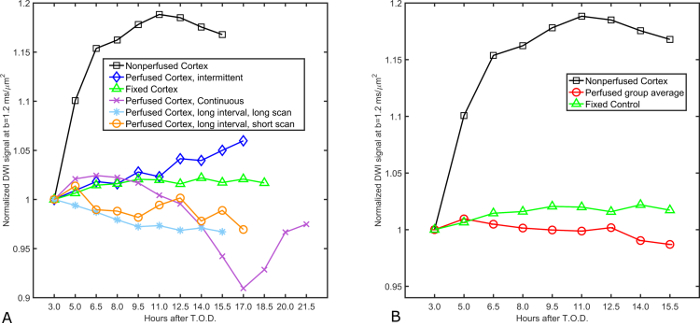
Figure 5: Diffusion signal stability in superfused acute cortical slices. (A) Normalized diffusion signal values in four acute slices subjected to differing superfusion paradigms are plotted over time for a period of up to 21.5 h following euthanasia. Slices remain within ± 5% of their initial diffusion signal measurement for a period of 15.5 h following euthanasia regardless of whether superfusion is continuous or intermittent and independent of the MR scan length (1.5 h or 4 min). Signal recordings taken from formaldehyde-fixed cortex serve as the positive control (n = 1) for stability due to the static, unchanging nature of fixed tissue samples. Conversely, diffusion signal measured in a live slice absent of superfusion support (n = 1) serves as a control for metabolic deficiency. Experiment parameters of the different superfusion trials are as follows: continuous (superfusion always on, time per scan = 1.5 h), intermittent (superfusion on for 10 min interval between scans, time per scan = 1.5 h), Long interval, long scan (superfusion on during scan, but paused for 10 min between scans, time per scan = 1.5 h), Long interval, short scan (superfusion on for 1.5 h interval between scans, time per scan = 4 min). (B) Analyzed data showing group means of the four live-slice superfusion experiments from panel (A). The diffusion signal profile from the grouped, superfused cortical slices exhibits little variation over time (2 ± 3% over 15.5 h) whereas the non-perfused control (n = 1) exhibits dramatic signal instability early in the experiment (15% by 6.5 h). This figure has been modified and reproduced with permission from the original article8. Please click here to view a larger version of this figure.
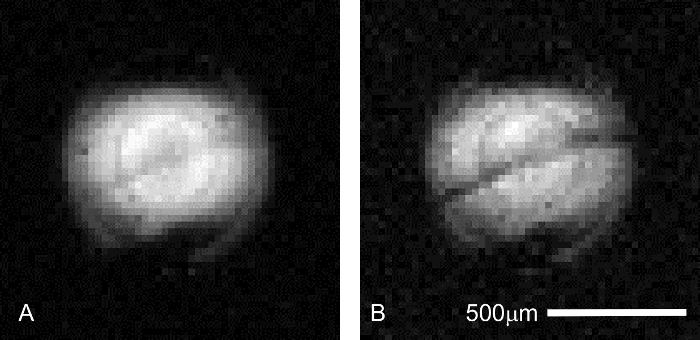
Figure 6: Confirmation of hippocampal slice placement during pilot imaging. Prior to running an extended MR microscopy session, correct placement of the sample is critical to ensure resources such as scanner time and expensive perfusate additives are not wasted. The pyramidal cell layer in the CA1 region of the hippocampus can be visualized in faster (4.3 min), lower resolution (31 μm x 31 μm in-plane) pilot scans to ensure the tissue of interest is placed correctly in relation to the micro-coil. Scan parameters common to both images are as follows: TR/TE = 2000/11.6 ms, Δ = 6 ms, δ = 1 ms, averages = 1. (A) b = 0 (227 effective) s/mm2. In this preliminary scan, the stratum pyramidale is only just visible as a grey, diagonal band centered in the coil's excitation profile. (B) b = 1,200 (1,860 effective) s/mm2. At higher diffusion weighting, interlamellar contrast increases as the pyramidal cell layer becomes darker than tissues in the adjacent laminae (above: stratum oriens; below: stratum radiatum). Please click here to view a larger version of this figure.
