The γδ T cell process was characterized and optimized for the production of the γδ T cell drug product. Process optimization included 1) lymphocyte enrichment using elutriation, 2) γδ T cell drug substance (DS) cell-specific expansion with zoledronic acid, 3) γδ T cell DS depletion of TCRαβ, 4) secondary expansion of the γδ T cell DS using K562-derived aAPCs, and 5) final DP harvest and formulation of product for administration or cryopreservation. After process optimization, confirmation runs were performed at scale using the material derived from three healthy donors to confirm cell-processing suitability. All data were analyzed and are summarized in Table 1, Table 2, and Table 3. The cells separated from the post-counterflow centrifugation fraction 2 (F2) yielded a pure lymphocyte population with an average of 99.23% CD45+ cells (reported as the frequency of total live gate) and excellent average viability of 95.80% (Table 1).
The γδ T-cell-specific expansion with zoledronic acid depended on the initial percentage of natural killer (NK) cells present in the lymphocyte fraction (F2) after elutriation. The enrichment of γδ T cell DS with TCRαβ depletion was consistent (Table 2). The γδ T cell DP manufactured from three healthy donors had an average of 0.11% ± 0.05% CD20+ B cells and 0.00% ± 0.00% TCR αβ+ T cells, thus meeting the release criterion of ≤1% of TCR αβ+ T cells. The average percentage of NK cells in the final product is 17.06% ± 26.19% and meets the release criterion of <35%. Additionally, the average percentage of T cell and NK cell lineage-negative cells in the final product was 0.48% ± 0.42% (Table 3). Cell surface staining and flow cytometric analysis were utilized to characterize the identity, purity, and process impurities of the DS and DP, as shown in Figure 2A–D.
The secondary expansion, achieved from the co-culture of the aAPC (K562CL6(CD3-CD137L:CD28-IL-15RA)) WCB and γδ T cell DS at a ratio of 10:1, generated a γδ T cell DP that met all release criteria, as shown in Table 4. In addition, the cells were stained and assessed by flow cytometry at Day 0-counterflow centrifugation F2 cells, Day 7-zoledronic acid-expanded T cells, Day 7-TCR αβ T cell depletion, Day 17-final DP for the following biomarkers cluster of differentiation (CD)3, TCRαβ, TCR γδ, CD45RA, CD45RO, CC chemokine receptor 7 (CCR7), programmed cell death protein-1 (PD-1), cytotoxic T lymphocyte-associated protein 4 (CTLA4), lymphocyte-activating gene 3 (LAG3), and T cell immunoglobulin and mucin domain-containing protein 3 (TIM3). Data shown in Figure 3 are averaged from three independent runs and demonstrate that cells have not reached exhaustion. The Moffitt CTF also developed a residual K562 assay to determine the DP impurities related to the K562-derived aAPCs (Figure 4).
The flow cytometric gating strategy used to characterize the percentages of the cell types was as follows: 1) gating on T and NK cell lineage-negative population (CD3–CD56–CD16–); 2) gate on CD71+ (transferrin receptor expressed in erythroid lineage and AML allowing for the detection of residual K562 cells). This gating strategy allowed the evaluation of the CD3–CD16–CD56–CD71+ cells, which are the aAPC (K562CL6(scFv-CD3-CD137;scFv-CD28-IL15-RA)) WCB (termed "residual K562" in Figure 4). This gating allows the enumeration of residual K562 in the final DP by multiplying the frequency of residual K562 by the total viable count (TVC) count of the DP (%CD71+ × DP TVC = Residual K562 cells in the DP). All flow cytometric data are reported as the frequency of live cells. Table 5 and Figure 4 provide the percentages of T cell and NK cell lineage-negative as well as residual K562 cells. A two-tailed t-test was performed to determine the statistical significance of the differences between these populations and revealed that there was a significant difference between WCB and γδ T cell DP and between WCB and γδ T cells (t = 0.0019 for T cell and NK cell lineage-negative; t < 0.0001 for Residual K562 and t = 0.0314 for T cell and NK cell lineage-negative; t < 0.0001for Residual K562) (Table 5).
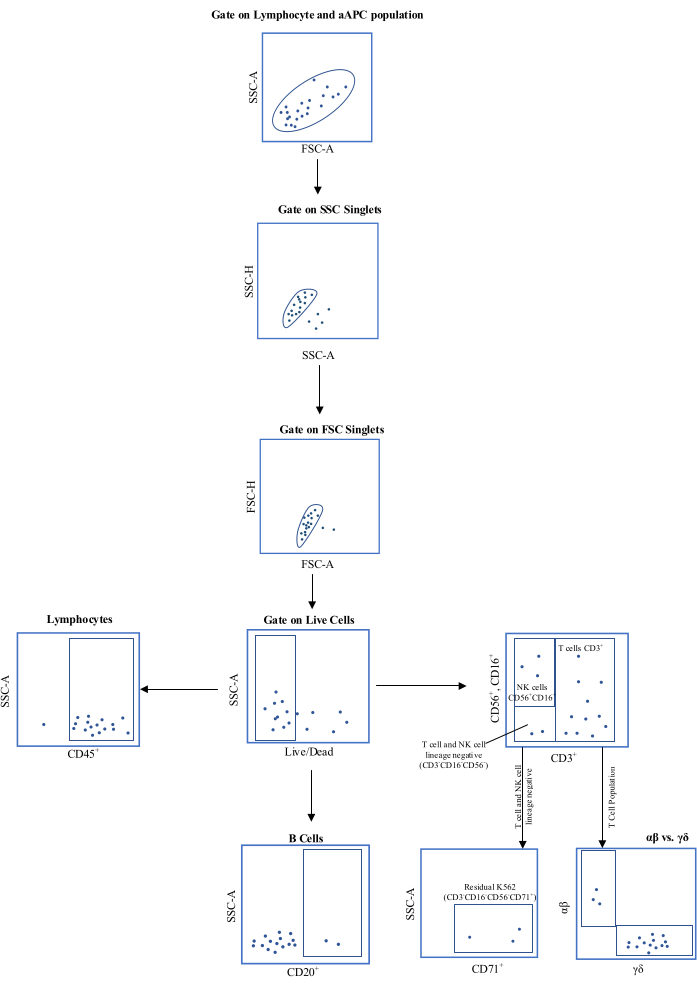
Figure 1: Schematic representation of the flow cytometric gating strategy. Abbreviations: aAPC = , artificial antigen-presenting cell; SSC-A = side scatter-area of peak; FSC-A = forward scatter-area of peak; SSC-H = side scatter-height of peak; FSC-H = forward scatter-height of peak; CD = cluster of differentiation. Please click here to view a larger version of this figure.
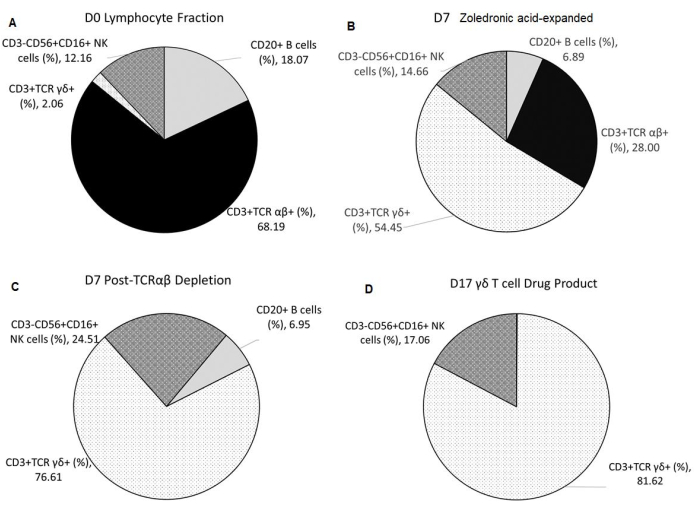
Figure 2: Composition of Starting Material, Intermediates, and Final Drug Product. All data shown are averaged from three independent runs. (A) Apheresis from healthy donors undergoes elutriation using the counterflow centrifugation device, resulting in F2 (lymphocyte-rich fraction), which is used as the starting material. (B) F2 undergoes Vγ9Vδ2 T cell-specific expansion for 7 days with 5 µmol/L of zoledronic acid and 300 IU/mL of IL-2 in 1 L of medium supplemented with 10% human AB serum. (C) TCR αβ T cell depletion is performed on the zoledronic acid-expanded product. (D) A highly pure γδ T cell Drug Product is harvested after a second 10-day expansion with irradiated aAPCs at a 1:10 ratio with 5 µmol/L of zoledronic acid and 300 IU/mL of IL-2 in 1 L of medium supplemented with 10% human AB serum. Abbreviations: NK = natural killer; CD = cluster of differentiation; TCR= T-cell receptor; IL = interleukin; aAPCs = artificial antigen-presenting cells. Please click here to view a larger version of this figure.
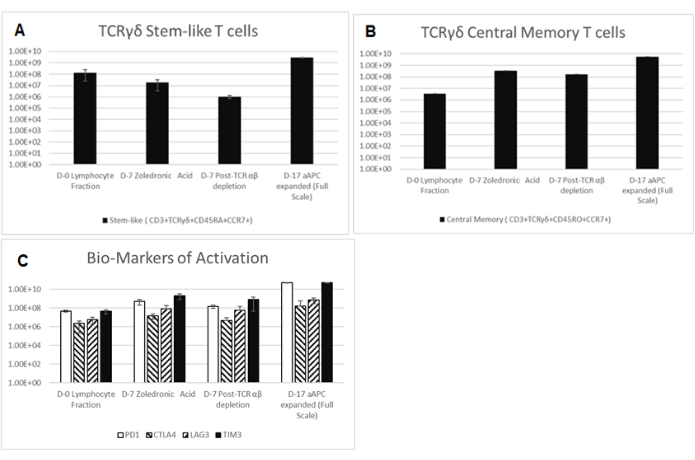
Figure 3: Biomarkers of Starting Material, Intermediates, and Final Drug Product. Cells are collected and stained for CD3, TCRαβ, TCR γδ, CD45RA, CD45RO, CCR7, PD-1, CTLA4, LAG3, and TIM3 at Day 0-Counterflow Centrifugation F2 cells, Day 7-zoledronic acid-expanded T cells, Day 7-TCR αβ T cell depletion, Day 17-Final Drug Product. All data shown are averaged from three independent runs. (A) Stem-like (CD3+, TCR γδ+, CD45RA+, CD45RO–, and CCR7+) shown as a total number of live cells. (B) Central memory (CD3+, TCR γδ+, CD45RA–, CD45RO+, and CCR7+) depicted as a percentage of CD3+ TCR γδ+ cells. Abbreviations: CD = cluster of differentiation; TCR= T-cell receptor; IL = interleukin; .CCR7 = CC chemokine receptor 7; PD-1 = programmed cell death protein-1; CTLA4 = cytotoxic T lymphocyte-associated protein 4; LAG3 = lymphocyte-activating gene 3; TIM3 = T cell immunoglobulin and mucin domain-containing protein 3. Please click here to view a larger version of this figure.
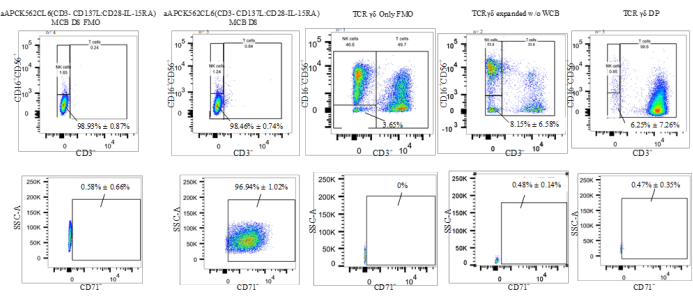
Figure 4: Representative data of a K562 residual assay(CD3–CD16–CD56–CD71+). Abbreviations: aAPC = artificial antigen-presenting cell; NK = natural killer cell; SSC-A = side scatter-area of peak; CD = cluster of differentiation; IL = interleukin; TCR = T-cell receptor; MCB =master cell bank ; FMO = fluorescence minus one; DP = drug product; WCB = working cell bank. Please click here to view a larger version of this figure.
| Process Steps | Parameters | Donors | Average | St. Dev. | |||
| Run 1 | Run 2 | Run 3 | |||||
| Post-Enrichment (Lymphocyte fraction F2) | TVC All Process Validations were seeded at 109 TVC | 1.00 X 109 | 1.00 X 109 | 1.00 X 109 | 1.00 X 109 | 0.00 | |
| Viability (%) | 98.6 | 96.6 | 92.2 | 95.8 | 3.27 | ||
| CD20+ B cells (%) | 15.6 | 23.4 | 15.2 | 18.07 | 4.62 | ||
| CD3+ T cell (%) | 80.04 | 66.7 | 76.1 | 74.28 | 6.85 | ||
| TCR αβ+ (%) | 77.59 | 58.03 | 68.96 | 68.19 | 9.8 | ||
| TCR γδ+ (%) | 2.48 | 1.59 | 2.1 | 2.06 | 0.45 | ||
| CD3–CD56+CD16+ NK cells (%) | 6.57 | 19.4 | 10.5 | 12.16 | 6.57 | ||
| T cell and NK cell lineage negative (%) | 13 | 13.7 | 13.4 | 13.37 | 0.35 | ||
Table 1: Summary of lymphocyte enrichment by elutriation reported as frequency of live cells. Abbreviations: TVC = total viable count; TCR = T cell receptor; CD = cluster of differentiation; NK = natural killer cell.
| Process Steps | Parameters | Donors | Average | St. Dev. | |||
| Run 1 | Run 2 | Run 3 | |||||
| 7-day Post Zoledronic acid Expansion (pre- TCRαβ depletion) | TVC | 3.69 X 109 | 1.79 X 109 | 1.42 X 109 | 2.3 X 109 | 1.22 X 109 | |
| Viability (%) | 99.2 | 82.6 | 89.8 | 90.53 | 8.32 | ||
| CD20+ B cells | 2.1 | 11.5 | 7.08 | 6.89 | 4.7 | ||
| CD3+ T cell (%) | 95.7 | 64.1 | 91.9 | 83.9 | 17.25 | ||
| TCR αβ+ (%) | 13.88 | 38.14 | 31.98 | 28 | 12.61 | ||
| TCR γδ+ (%) | 81.44 | 24.93 | 56.98 | 54.45 | 28.34 | ||
| CD3–CD56+CD16+ NK cells (%) | 3.59 | 33.1 | 7.28 | 14.66 | 16.08 | ||
| T cell and NK cell lineage negative (%) | 0.67 | 2.7 | 0.82 | 1.4 | 1.13 | ||
| Post- TCRαβ depletion | TVC | 1.81 x 109 | 4.95 X 108 | 3.80 X 108 | 8.95 X108 | 7.94 X 108 | |
| Cell viability (%) | 98.8 | 87.6 | 89.8 | 92.07 | 5.93 | ||
| CD20+ B cells | 2.26 | 12 | 6.59 | 6.95 | 4.88 | ||
| CD3+ T cell (%) | 95.8 | 45.3 | 89.7 | 76.93 | 27.56 | ||
| TCR αβ+ (%) | 0 | 0.001 | 0.001 | 0.001 | 0.001 | ||
| TCR γδ+ (%) | 95.61 | 45.07 | 89.16 | 76.61 | 27.51 | ||
| CD3–CD56+CD16+ NK cells (%) | 3.85 | 59.9 | 9.79 | 24.51 | 30.79 | ||
| T cell and NK cell lineage negative (%) | 0.34 | 1.72 | 0.45 | 0.84 | 0.77 | ||
| TCR αβ+ TVC | 0.00 | 4.95 x 103 | 3.8 X 103 | 2.92 X 103 | 2.59 X 103 | ||
| TCR γδ+ TVC | 1.73 X 109 | 2.23 X 108 | 3.39 X 108 | 7.64 X 108 | 8.39 X 108 | ||
| CD3–CD56+CD16+ NK TVC | 6.97 X 107 | 2.97 X 108 | 3.72E+07 | 1.35 X 108 | 1.42 X 108 | ||
Table 2: Summary of γδ T cell expansion with zoledronic acid and instrument enrichment reported as frequency of live cells. Abbreviations:TVC = total viable count; TCR = T cell receptor; CD = cluster of differentiation; NK = natural killer cell.
| Product Attributes | Parameters | Donors | Average | St. Dev. | |||
| Run 1 | Run 2 | Run 3 | |||||
| Day 0 γδ T Cells | 2.48 X 107 | 1.59 X 107 | 2.10 X 107 | 2.06 X 107 | 4.47 X 107 | ||
| Day 7 post enrichment γδ T Cells | 1.73 X 109 | 2.23 X 108 | 3.39 X 108 | 7.64 X 108 | 8.39 X 108 | ||
| Fold Expansion at Day 7 | 69.76 | 14.03 | 16.14 | 33.31 | 31.58 | ||
| TVC at harvest* | 8.14 X 1010 | 1.67 X 1010 | 6.84 X 1010 | 5.55 X 1010 | 3.42 X 1010 | ||
| Cell viability (%) | 92.8 | 85.5 | 87.3 | 88.53 | 3.80 | ||
| CD20+ B cells (%) | 0.12 | 0.06 | 0.15 | 0.11 | 0.05 | ||
| CD3+ T cell (%) | 97.8 | 52 | 97.5 | 82.43 | 26.36 | ||
| TCR αβ+ (%) | 0 | 0.001 | 0 | 0.00 | 0.00 | ||
| TCR γδ+ (%) | 97.51 | 50.13 | 97.21 | 81.62 | 27.27 | ||
| CD3–CD56+CD16+ NK cells (%) | 2.16 | 47.3 | 1.71 | 17.06 | 26.19 | ||
| T cell and NK cell lineage negative, CD71+ Residual K562 (%) | 0.018 | 0.61 | 0.82 | 0.48 | 0.42 | ||
| Total γδ T cells at Harvest | 7.93 X 1012 | 8.38 X 1011 | 6.65 X 1012 | 5.14 X 1012 | 3.78 X 1012 | ||
| Total Fold Expansion of γδ T cells (From day 0 to Harvest) | 3.20 X 105 | 5.27 X 104 | 3.17 X 105 | 2.30 X 105 | 1.53 X 105 | ||
| *Process Validation was scaled down to flask with 5 X 106 γδ T cell and 50 X106 irradiated aAPCs. Numbers reported are for a projected full scale run if 24 flasks are seeded from the D7 drug substance was used. | |||||||
Table 3: Summary of γδ+ T cell co-culture with aAPCs and expanded γδ+ T cell harvest reported as frequency of live cells. *Process validation was scaled down to one closed-system bioreactor (1 L capacity) with 5 × 106 γδ T cells and 50 × 106 irradiated aAPCs. Numbers reported are for a projected full-scale run if 24 flasks are seeded from the D7 drug substance. Abbreviations: aAPCs = artificial antigen-presenting cells; TVC = total viable count; TCR = T cell receptor; CD = cluster of differentiation; NK = natural killer cell.
| Test Parameter | Acceptance Criteria | Resultados | ||
| Validation 1 | Validation 2 | Validation 3 | ||
| Viability | ≥ 70% | 92.80% | 85.50% | 87.30% |
| Mycoplasma | Negative | Negative | Negative | Negative |
| Sterility | No Growth Final (14 days) | No Growth Final (14 days) | No Growth Final (14 days) | No Growth Final (14 days) |
| Gram stain | No organisms seen (NOS) | NOS | NOS | NOS |
| Endotoxin | ≤ 2 EU/mL | <0.50 EU/mL | <0.50 EU/mL | <0.50 EU/mL |
Table 4: Summary of quality control release testing results for the γδ T cells.
| Residual K562 Assay | K562 | WCB | γδ Only | γδ + WCB Product | ||||
| T and NK cell lineage neg. % | Residual K562 % | T and NK cell lineage neg. % | Residual K562 % | T and NK cell lineage neg. % | Residual K562 % | T and NK cell lineage neg. % | Residual K562 % | |
| 99.4 | 98.8 | 98.7 | 96.83 | 3.49 | 0.58 | 0.48 | 0.07 | |
| 99.2 | 98.31 | 99.5 | 98.21 | 12.8 | 0.38 | 3.87 | 0.71 | |
| 98.9 | 98.6 | 97.6 | 95.55 | N/A | N/A | 14.4 | 0.63 | |
| 99.2 | 98.9 | 97.9 | 96.53 | N/A | N/A | N/A | N/A | |
| 98.7 | 98.3 | 98.6 | 97.6 | N/A | N/A | N/A | N/A | |
| Average | 99.08 | 98.58 | 98.46 | 96.94 | 8.15 | 0.48 | 6.25 | 0.47 |
| St. Dev. | 0.28 | 0.27 | 0.74 | 1.02 | 6.58 | 0.14 | 7.26 | 0.35 |
Table 5: T cell and NK cell lineage-negative and residual K562 percentages reported as frequency of live cells. Abbreviations: NK = natural killer cell; WCB = working cell bank.
