When a patient is admitted to the EMU, a simultaneous scalp EEG and video are recorded. One purpose of the EEG monitoring by a neurologist is to evaluate for epileptiform discharges, which can potentially inform the localization of the seizure onset. When extraordinary dynamics of specific EEG channels are distinguished, the electrode locations can be associated with seizure localization. During the interictal period, interictal epileptiform discharges (IEDs), including spikes and sharp waves, are traditionally considered as markers of areas of epileptogenicity. Furthermore, the obtained recordings of interictal EEG-fMRI data can be advantageous to understand and localize the seizures. To validate this EEG-fMRI recording and EEG processing protocol, we evaluate the quality of the EEG by comparing the postprocessed EEG to the one from the EMU, and we confirm that the same distinguishable EEG characteristic is observed in both cases.
Focal delta slow activity is typically suggestive of an underlying brain structural lesion or an area where the neurons are not functioning as expected, which is often observed after strokes, head injuries, brain infections, or dementia. However, it is not uncommon for patients with focal epilepsy to demonstrate focal delta activity near or at the site of their epileptogenic zone. In addition, although focal delta activity is less specific than IEDs, it can specify localized structural pathology corresponding to seizure onset in epilepsy12. Furthermore, focal interictal slow waves in EEGs correspond to focal BOLD activation on fMRI that matches the epileptogenic area in patients with partial epilepsy13.
It is notable that, in temporal lobe onset epilepsy, a type of delta activity called temporal intermittent rhythmic delta (TIRDA) is sometimes present, and it is considered an IED equivalent14. On the contrary, temporal intermittent polymorphic delta (TIPDA) is not considered an IED equivalent15. In the processed EEG data, clear focal left temporal slow waves (TIPDA) are present, which is observed from the EEG recorded at the EMU (Figure 7). Although this delta activity is not IED equivalent, it suggests left temporal neuronal dysfunction.
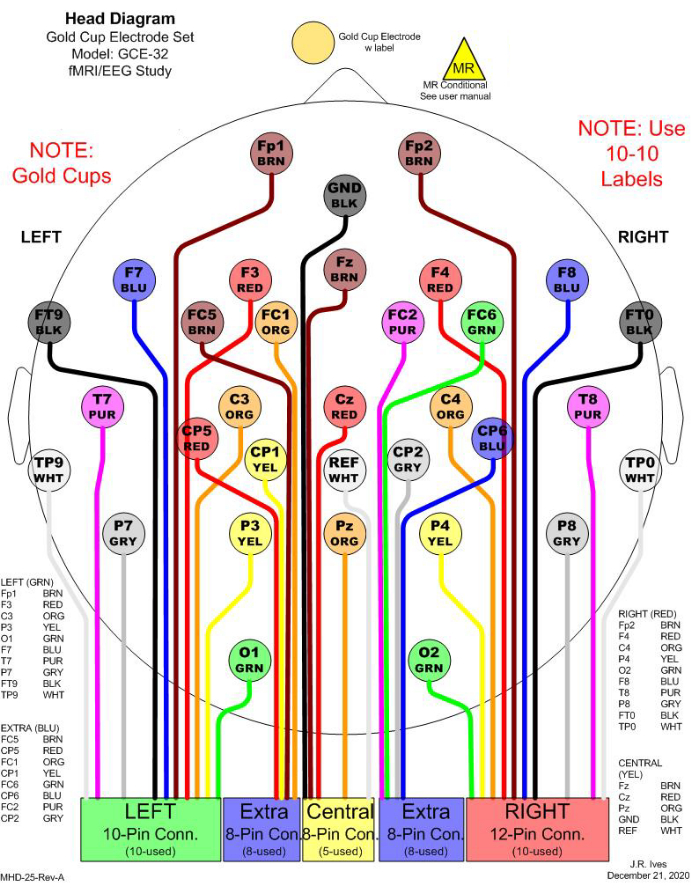
Figure 1: An example of 32 electrode selections for simultaneous EEG-fMRI recording. In the clinic, 21 channels are commonly considered for EEG monitoring. To fulfill a minimum number of electrodes to conduct EEG source imaging (ESI), 11 additional channels are included to cover the head entirely. All electrodes are gold cups to avoid MR effects. In the figure, different colors are used to distinguish different electrodes, and the colors match the physical cable colors. Each rectangular box in the bottom indicates one junction to be connected to a harness, which will be connected to an amplifier for recording. Please click here to view a larger version of this figure.
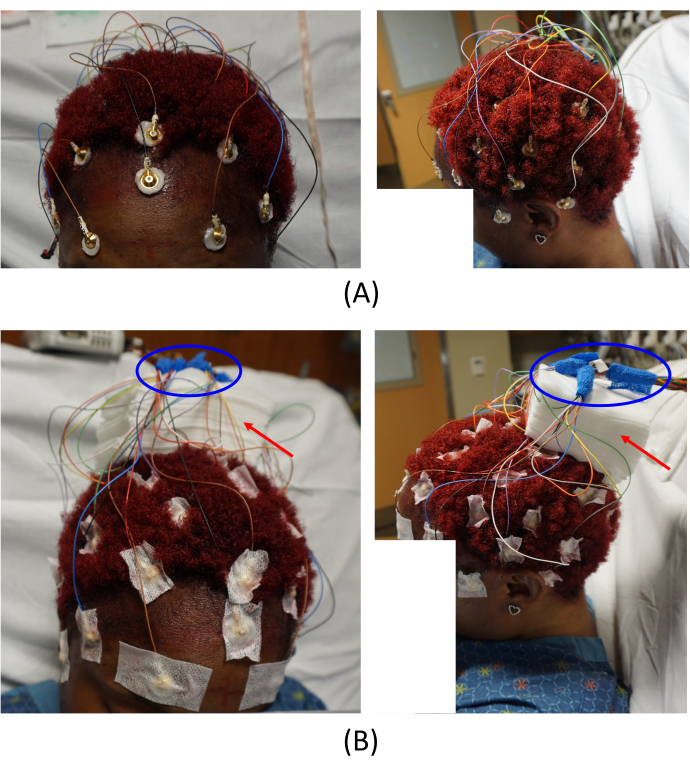
Figure 2: Electrode placements. (A) Placement of the electrodes on the patient's scalp and (B) arrangement of the cable junctions. The left images in (A) and (B) provide a top-front view, and the right images provide a left-side view of the patient. The red arrows in (B) indicate the placement of gauze pads. This helps to avoid imaging artifacts. The areas circled in blue in (B) show how the cable junctions are arranged. Please click here to view a larger version of this figure.
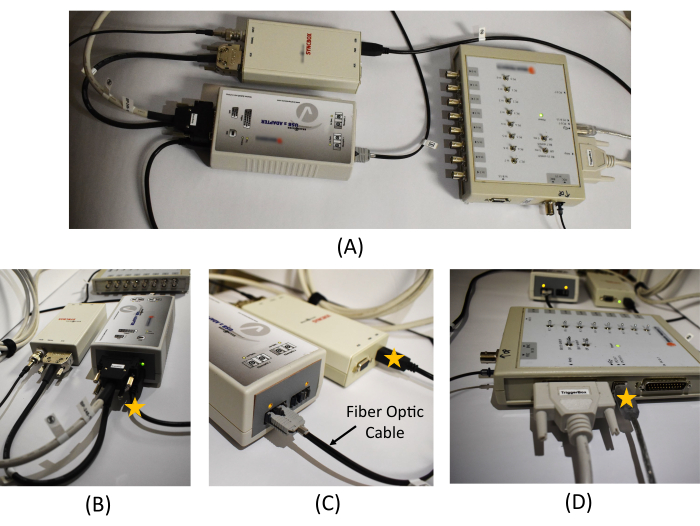
Figure 3: Equipment connection in the monitoring room. (A) An overview of the USB 2 adapter, Syncbox, and Triggerbox connection. Detailed picture of (B) the USB 2 adapter and Syncbox cable connections, (C) the Syncbox and the fiber optic cable connection, and (D) the cable connections in the Triggerbox. The star marks on (B), (C), and (D) show the location of the USB cables to be connected to the recording PC. A schematic diagram of the EEG recording system and the connections required between the hardware is provided in Figure 1 in Mullinger et al.7. Please click here to view a larger version of this figure.
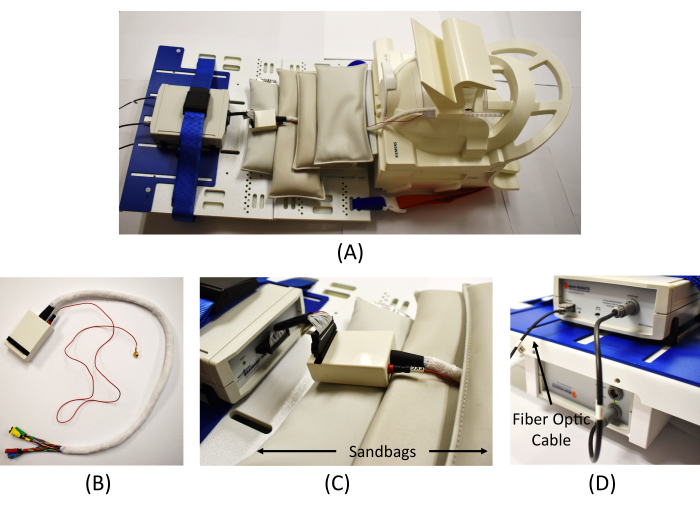
Figure 4: Equipment connection in the scanning room. (A) An overview of the EEG amplifier connection in the scanner. (B) Wrapped cables from the interface box to connect the EEG electrodes (the red cable is for the ECG measure). (C) Connection of the interface box and the EEG amplifier and MR safe sandbags placed to reduce MR artifacts. (D) Connection of the amplifier (top) and the battery (bottom) and connection of the fiber optic cable from the Syncbox in the monitoring room to the amplifier. Please click here to view a larger version of this figure.
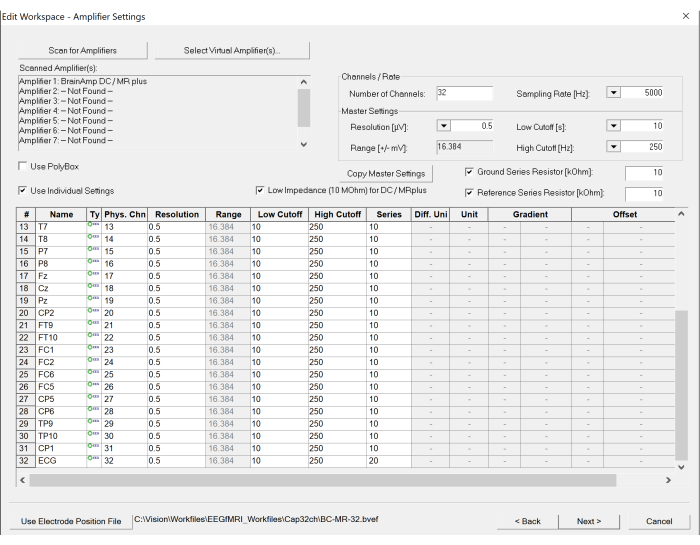
Figure 5: Screenshot of workspace settings on the EEG recording software. The number of channels and sampling rate can be set under the amplifier settings. In addition, the specification of each channel can be modified, if necessary, by clicking the table at the bottom. Please click here to view a larger version of this figure.
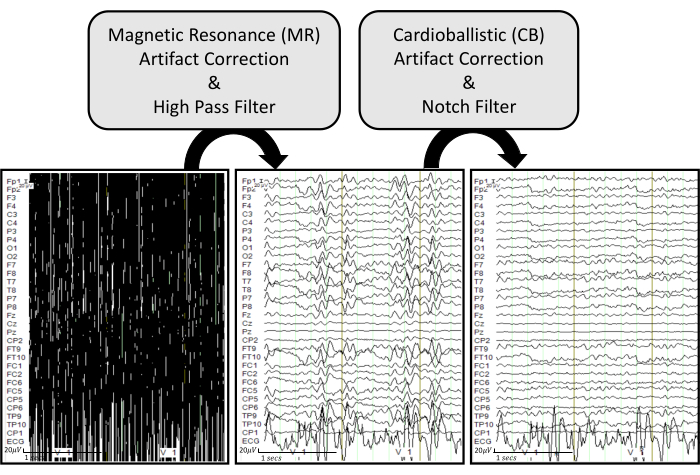
Figure 6: EEG artifact removal pipeline with representative examples. The raw EEG traces are displayed in the bottom left. The bottom middle plot shows EEG traces after applying MR artifact correction and a high pass filter of 0.5 Hz on the raw EEG. The bottom right plot displays EEG traces after applying CB artifact correction and a notch filter of 60 Hz on the processed EEG. The EEG traces are displayed under common ground mode to effectively visualize how each process influences each recorded channel. Please click here to view a larger version of this figure.
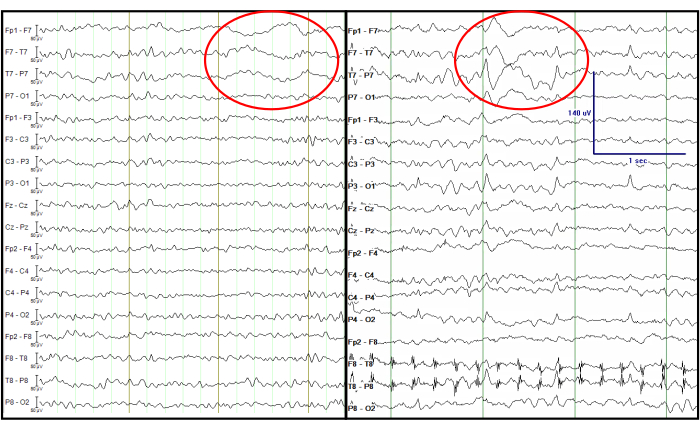
Figure 7: Comparison of the processed EEG from a simultaneous EEG-fMRI recording (left) and an EEG recorded at the EMU (right). The red circle indicates focal left temporal slow waves at the same channels. The EEG traces are displayed in a double banana format, which is traditionally considered in the clinic. Please click here to view a larger version of this figure.
