In this study, a simple and rapid method for isolating leukocytes from 1 mL of whole blood and obtaining CL fingerprinting by MALDI-TOF/MS has been described (see Figure 2). Figure 3 shows the comparison of representative CL fingerprinting of leukocytes, obtained from control subjects and BTHS young boys, in the CL and MLCL mass (m/z) range. Table 1 lists CL and MLCL species detected in these mass spectra.
Defects in the TAFAZZIN gene typically determine a lipid profile specific for the BTHS, i.e., the appearance of MLCL and CLi forms together with the reduction of CLm forms in the CL fingerprint. The lipid profile of leukocytes of control subjects typically exhibits only two molecular species of CLm (upper panel of Figure 3). The only peaks of interest present in this mass spectrum are CLm species: tetralinoleoyl CL (18:2)4 at m/z 1,448.0 and CL (18:2)3 (18:1)1 at m/z 1,450.0. This method allows their visualization in the MALDI lipid profile so that the two CL species can be easily identified and measured in the healthy phenotype.
The representative CL fingerprinting of a boy affected by BTHS shows a different pattern of MALDI signals (lower panel of Figure 3). The signals attributable to CLm species are lower, while peaks assigned to two CLi species (at m/z 1,404.0 and 1,430.0) and two MLCL species (at m/z 1,165.8 and 1,191.8) are also found (see Table 1). In summary, data in Figure 3 clearly show that the mitochondrial CL and MLCL species can be readily detected by MALDI-TOF/MS analyses of leukocytes.
A previous study has demonstrated that the (MLCL + CLi)/CLm ratio calculated in lipid profiles of leukocytes obtained by MALDI-TOF/MS can be used as a diagnostic parameter for BTHS28. In that study, CL fingerprinting of leukocytes isolated from healthy subjects and BTHS boys was compared28. Here, results obtained from the MALDI lipid profile of leukocytes isolated from 11 pediatric heart failure patients (one BTHS-affected and 10 non-BTHS-affected) were added.
Figure 4 shows calculated (MLCL + CLi)/CLm ratios in MALDI mass spectra of lipid mini-extracts of leukocytes from nine BTHS patients, 10 non-BTHS-affected (i.e., heart failure patients), and 22 healthy subjects; the ratio has been calculated by considering the area of CL and MLCL peaks detected in the mass spectra, as described, but intensities can also be used with similar results (data not shown).
The (MLCL + CLi)/CLm ratio for BTHS-patients was 7.2 ± 2.9, while those calculated for healthy subjects and heart failure patients were 0.19 ± 0.10 and 0.13 ± 0.07, respectively (mean ± SD). It can be seen that control groups (both healthy subjects and heart failure patients) and BTHS-patients are separated by more than one order of magnitude, showing that this method has strong diagnostic power.
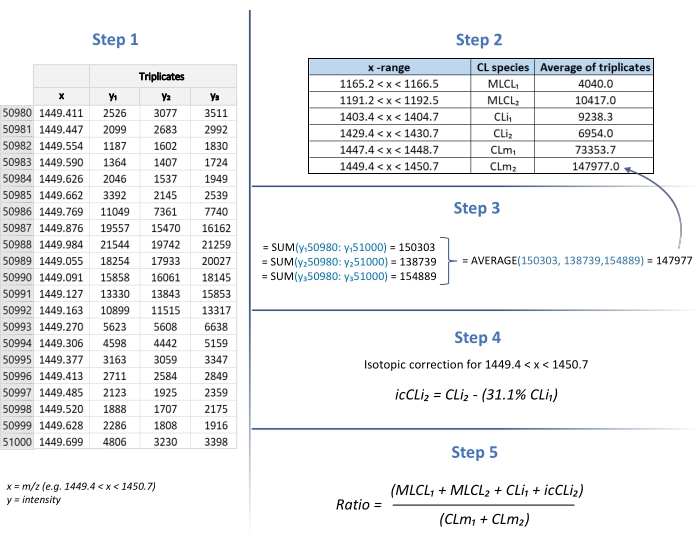
Figure 1: (MLCL+CLi)/CLm ratio determination. The calculation of the (MLCL + CLi)/CLm ratio is performed using the Excel program. Step 1: Table of m/z (x) / intensity (y) for species of interest (in triplicates). Step 2: Table of x-ranges to calculate each peak area. Step 3: Calculation of SUM and AVERAGE of y1, y2, and y3 values (triplicates). Step 4: Calculation of isotopic correction. Step 5: Calculation of the (MLCL+CLi)/CLm ratio. Please click here to view a larger version of this figure.
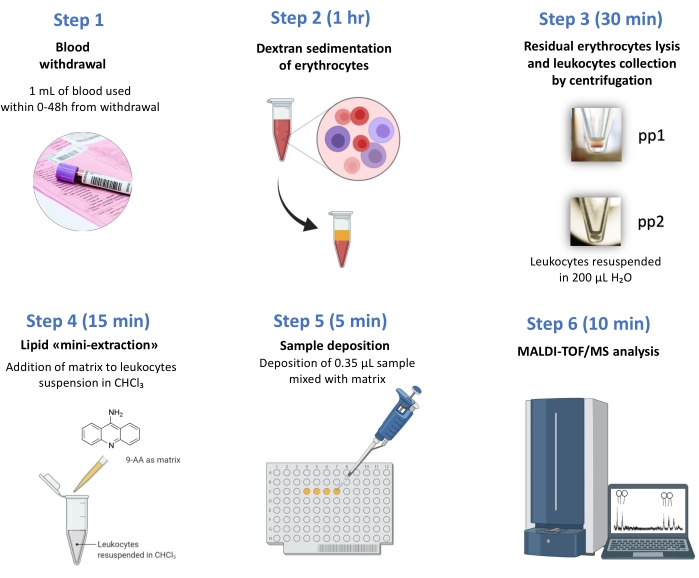
Figure 2: Work-flow chart. From the blood withdrawal to the test results, only 2 h are necessary. MALDI-TOF/MS-based BTHS diagnosis in few steps: (1) Blood withdrawal; (2) Dextran sedimentation of erythrocytes, (3) residual erythrocytes lysis (pp1) and leukocytes collection (pp2) by centrifugation, (4) lipid "mini-extraction", (5) sample deposition, (6) MALDI-TOF/MS analysis. Please click here to view a larger version of this figure.
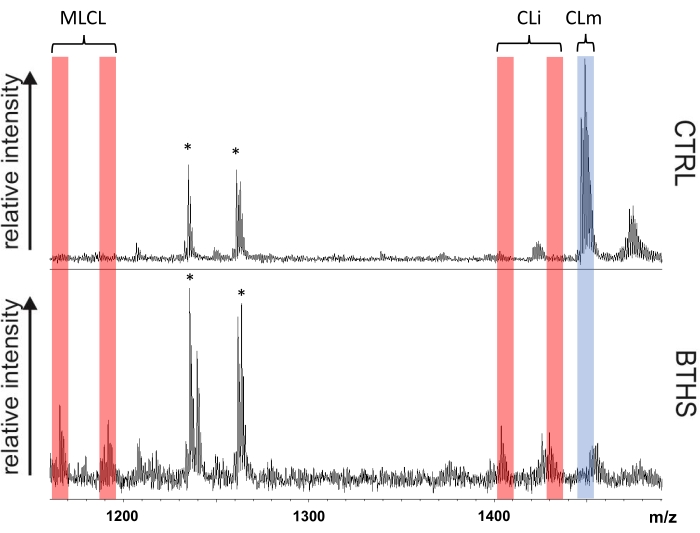
Figure 3: BTHS diagnostic leukocyte CL fingerprints. Comparison of cardiolipin fingerprints of leukocytes isolated from a control subject (CTRL) and a representative Barth syndrome patient (BTHS) is shown. Red bands highlight peaks of the immature form of cardiolipin (CLi) and monolysocardiolipin (MLCL) species, while the blue band marks the peaks of the mature forms of CL (CLm). Signals labeled with an asterisk refer to gangliosides and are not of interest to this study. Please click here to view a larger version of this figure.
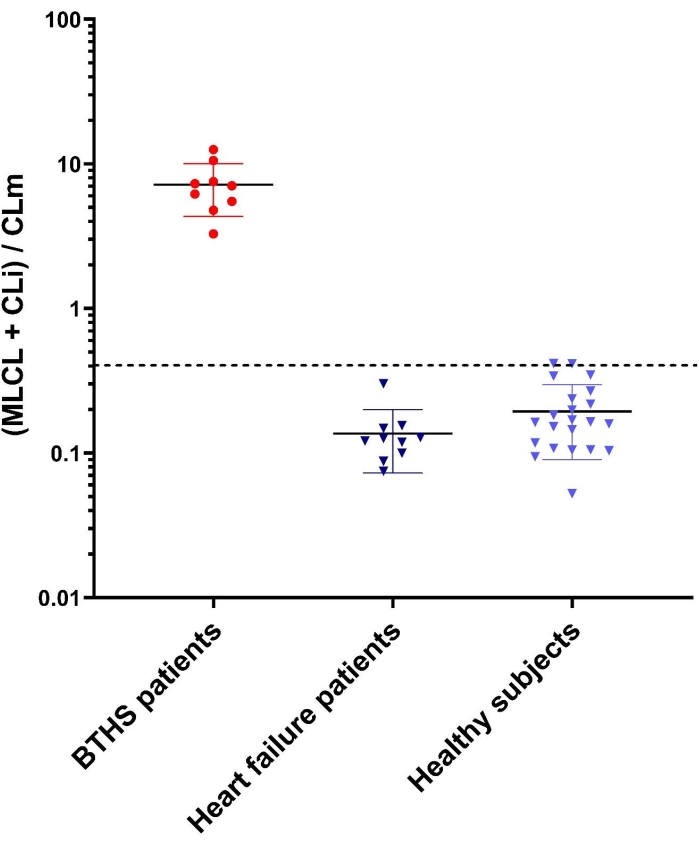
Figure 4: (MLCL + CLi)/CLm ratios in controls and BTHS patients. Error bars indicate standard deviations obtained from the mean of measurements of all subjects for each of the three groups: nine BTHS patients, 10 non-BTHS-affected heart failure patients, and 22 healthy subjects. Each sample was analyzed by MALDI-TOF/MS (in triplicate). The y-axis shows a logarithmic scale. The upper cut-off value of controls, calculated as in references22,28 is 0.4. Please click here to view a larger version of this figure.
| m/z [M-H]– | Assignment |
| 1165.8 | MLCL 52:2 |
| 1191.8 | MLCL 54:1 |
| 1404.0 | CLi 68:2 |
| 1430.0 | CLi 70:3 |
| 1448.0 | CLm 72:8 |
| 1450.0 | CLm 72:7 |
Table 1: List of detected peaks assigned to CL and MLCL species in the MALDI-TOF mass spectra.
