The methodology outlined in the protocol allows the collection of fMRI images while the volunteer is performing the task in real-time in the magnet. Experiments were performed in the Bay 1 facility of the Massachusetts General Hospital Athinoula A. Martinos Center for Biomedical Imaging, using a 3T full-body magnetic resonance scanner. Figure 2 and Figure 3 show the placement of the MR_CHIROD on the table and the patient in place operating it. In Figure 3, a volunteer is in the scanner bore with his/her head placed at the isocenter of the magnet, which is the correct position for brain imaging. Figure 4 shows a schematic of the system components and connections, which are set up during the initial phases of the process. During an fMRI session, not only are the images collected, but also a real-time trace of the actual strokes of the device as the person in the magnet bore is operating it are obtained. Typical results are shown in Figure 5. The use of controlled pneumatic pressure allows precise control of the constant reaction force provided by the MR_CHIROD v3.
Figure 5A–C shows typical areas of activation during gripping/releasing of the device, using the results of the BOLD technique during fMRI scanning. Red arrows show activation in the M1 region (primary motor cortex) and green areas show the SMA (supplementary motor cortex). Figure 5D shows the measured displacement during gripping/releasing, which was performed against the MR_CHIROD’s resistance force. Figure 5E shows activation over time at a single voxel, chosen from within the somato-sensory area. The response corresponds with the subject’s activity, elevated activation occurring during gripping/releasing, and reduced activation when the subject is resting.
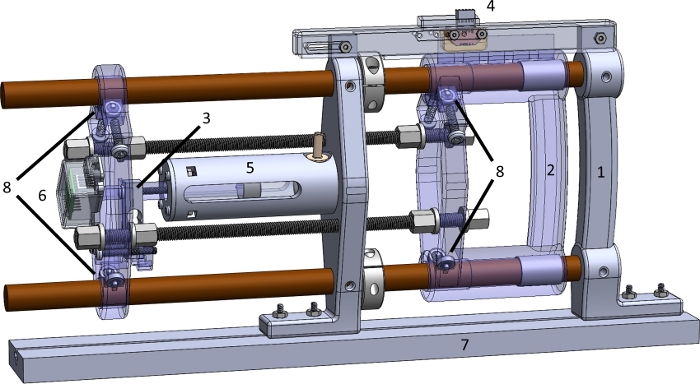
Figure 1: The parts of the MR_CHIROD v3 device. (1) Fixed handle; (2) Sliding handle; (3) Force sensor; (4) Position encoder; (5) Glass-graphite cylinder-piston unit; (6) Shielded load cell amplifier; (7) MR table mounting slot (mockup); (8) Ball bearings with acetyl races and glass balls. Please click here to view a larger version of this figure.
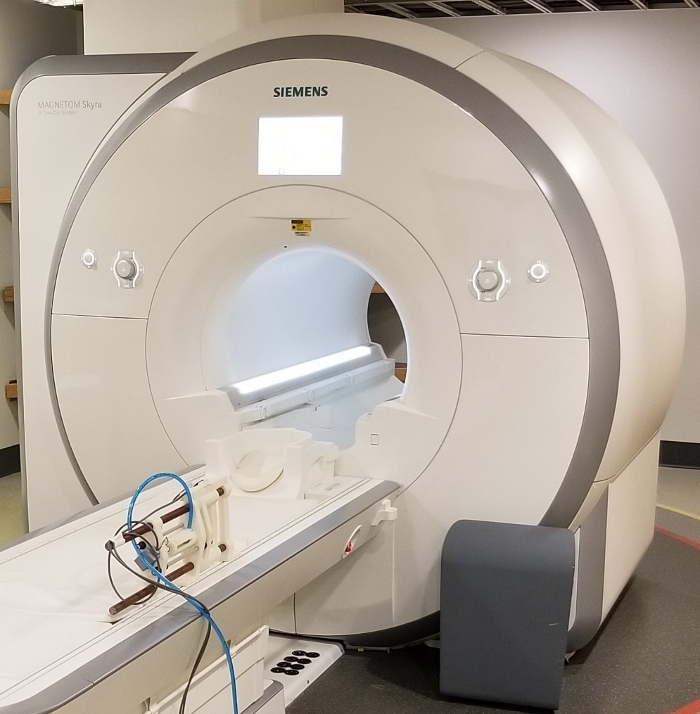
Figure 2: View of the MR_CHIROD v3 securely attached at the scanner bed. This configuration allows the person to operate the MR_CHIROD without supporting any of its weight. The device may be positioned for left or right hand. Shielded cables are grounded at penetration panel, pneumatic tube exits via a pass through tube in the penetration panel. Please click here to view a larger version of this figure.
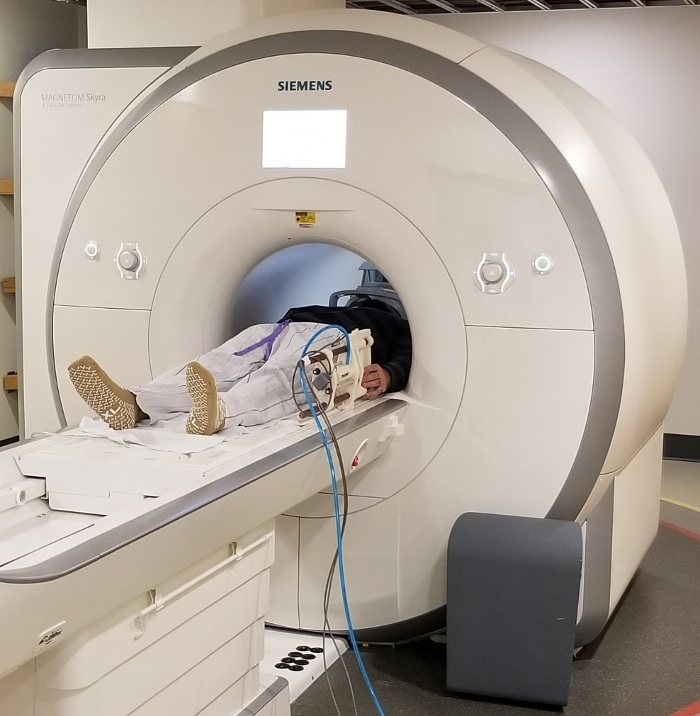
Figure 3: View of the MR_CHIROD v3 relative to a patient. A volunteer is resting with his hand in position near the handles of the device. The volunteer is placed in the correct position at magnet isocenter for brain imaging. Please click here to view a larger version of this figure.
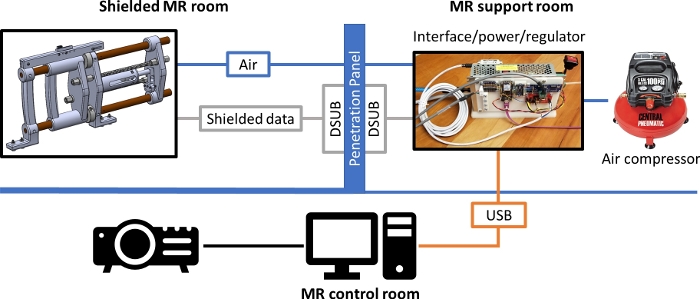
Figure 4: Schematic diagram of MR_CHIROD set up for operation in an MR scanner room. The shielded cables carrying the signals for the position and velocity data and for the force sensor, as well as the pneumatic tubing pass through the penetration panel which serves as the grounding reference level. Please click here to view a larger version of this figure.
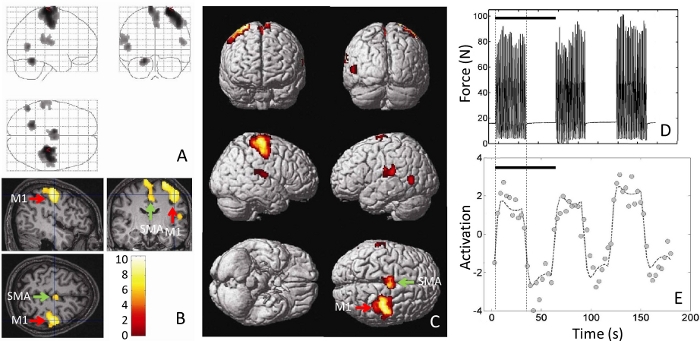
Figure 5: Typical results from performing a motor task (squeezing the handles of a MR_CHIROD). Shown are (A) the fMRI brain activations, superimposed as blobs on an outline of the brain, (B) as pseudo-color on a three-dimensional cross-sectional view of the volunteer’s anatomical brain scan, and (C) as pseudo-color rendered on a brain template. M1 = Primary motor cortex. SMA = Supplementary motor area. (D) Actual force output, measured in units of force (Newton, N) as a function of time. The force output is the actual record of the volunteer’s squeezing and is recorded in real time by the MR_CHIROD. (E) The single-voxel time course of activation is shown, chosen from a voxel at the somatosensory area at the location of the cross-hairs in (B). Black bars in (D) and (E) correspond with a 60 s stimulus/rest period. Please click here to view a larger version of this figure.
