The study was approved by the Ethical Committee of Region Midtjylland (1-10-72-259-21) and performed in compliance with the Helsinki Declaration and its amendments.
1. Fabrication of a custom-made spacer (optional)
NOTE: A custom-made 3D-printed spacer may be used during image acquisition to standardize the positioning of the camera head. The spacer is not mandatory for the recording of the fluorescence images.
- Design of the spacer
- Design a spacer that fits the camera head of the intraoral fluorescence camera. To do so, perform a scan of the camera head with a digital scanner. Import the scan into dedicated software.
- Design the spacer to fit the camera head with the desired morphology and positioning distance to the camera head (i.e., 4 mm). Export as an STL file (an example of a design is attached as Supplemental File S1).
- Additive manufacturing of the spacer
- Open the printer-associated additive manufacturing software, and select the basic settings. Click on Printer | Select the available 3D printer | Next | Shape: Clear | Next | Print mode: 50 microns | Next | Build Style: Standard | Next.
- Import the STL file by clicking on File | Import | Select the STL file | Open.
- Define the position of the spacer on the print platform; click on Transform, and drag the spacer to a corner of the platform as close to the surface of the platform as possible.
- To print additional spacers, click on Copy | Linear pattern. Adjust the count and distance to fit additional objects to the print platform, and click on Set.
- To design the support of the objects, click on Smart support | Style: General | Generate | Type: Gate | Create support.
- Send the print job to the 3D printer. Click on Add to queue. The software automatically performs a quality check of the STL file to identify errors when adding to the queue. Then, click on Add to queue | Job name | F4X | Add to queue.
- Mount a clean print platform on the 3D printer, and add an appropriate resin. Click on Start job, and scan the QR code of the resin. Confirm that the print platform is empty and clean, that the resin tray is full, and that the resin has been stirred before addition. Click on Start job.
- When the print job is finished, remove the spacers from the print platform.
- Clean the spacers in an ultrasound bath with isopropanol for 3 min. Repeat the cleaning using fresh isopropanol. Air-dry the spacers.
- Secure the total polymerization of the material by polymerizing the spacers in a post-curing oven for 10 min.
- Remove the support material, and stain the spacers to prevent light from penetrating through the material.
2. Plaque disclosure and image acquisition
- Mount the custom-made spacer on the fluorescence camera (optional). Connect the intraoral camera to a computer, and open the camera software.
- Click on Patient | New patient to create the patient in the system. Fill out the patient information. Click on Patient | Save to save the patient data. Click on Video. The intraoral camera is now ready to use.
- Dim the room lights.
- Apply a red disclosing dye (i.e., 5% erythrosine) with a cotton pellet on the tooth surfaces of interest to disclose the plaque.
- Instruct the patient to rinse with water for 10 s to remove excess dye. Remove any gingival stain using a cotton pellet. Air-dry each tooth for 3 s.
- Place the intraoral camera in a horizontal position in front of the tooth of interest, with the spacer touching the gingiva/adjacent teeth. Acquire the fluorescence image by pressing the camera button.
NOTE: Ensure that the entire tooth surface of interest is in focus and captured in the image without including antagonist or contralateral tooth surfaces. - Repeat steps 2.4-2.6 for all the teeth of interest.
- Mark all the images in the camera software. Click on Save images/videos in the menu.
NOTE: Make sure that the images are saved in "plaque"-mode and not in "caries"-mode. The symbol P/C in the menu indicates the current mode. - To export the images, go to the Viewer. Choose the images to be exported. Click on File | Export (save as…) | All images of the patient to export the images. In the export window, choose the following settings: Mode: Standard | Export path: Choose the desired folder | Image type selection: Check off the left box | Image state: Original data. Expand the export window to display more options. Select the following: File name contains: Cardnumber OR User input OR Patient name | Format: TIF. Click on OK to export the images.
- Alternatively, set up an automated file export prior to imaging. Click on Options | Show configuration | Modules | Viewer | Export/Email | Export options | Mode: Autoexport| Export path: Choose the desired folder | Image state: Original data. Select the following: File name contains: Cardnumber OR User input OR Patient name | Format: TIF. Click on OK to set up the default export settings. When the automated file export is set up, the images will automatically be exported when saved (step 2.8).
3. Digital image analysis
NOTE: The digital image analysis can be performed at any time after the image acquisition. Batches of up to 1,000 fluorescence images can be processed in parallel. If the analysis of large image batches exceeds the computing power, the image size may be reduced prior to analysis.
- Quantification of the total tooth area
- Rename all the images with sequential index numbers (i.e., Planimetry_001, Planimetry_002,…). Import the fluorescence image series into a dedicated image analysis software (i.e. Daime15) in Red-Green-Blue (RGB) mode by clicking on File | Import images | Import as color.
- Perform a threshold-based segmentation of the image series by clicking Segment | Automatic segmentation | Custom threshold. Set the "Low" threshold above the intensity of the oral soft tissues (i.e., 80). Leave the "High" threshold at 255. Thus, only the teeth (both clean and plaque-covered areas) are recognized as objects in the software. Click on Apply | OK | Segment! to initiate the segmentation.
- Open the visualizer by double-clicking on the name of the image series. Enter the object editor (OBJ). Perform a visual quality control of the segmented images, and delete artifacts by rejecting and deleting such objects.
- Merge the remaining objects in all the images (In all images | Merge selected objects). Now, there is one object per image. Quantify the total tooth area in each image (Analysis | Measure objects | Clear all | Pixels). Export the data.
- Quantification of the plaque-covered areas
- Import the fluorescence image series again into the software, this time with split red, green, and blue color channels (File | Import images | Import as grey). Close the blue channel images. Transfer the object layer from the RGB images to the red channel images (Segment | Transfer object layer).
- Delete non-object pixels in the red channel images using the object editor (In all images | Delete non-object pixels (voxels)). Soft tissues are now removed from the images.
- To enhance the contrast between plaque-covered and clean tooth areas, multiply the red channel image series by a factor of two (Edit | Image calculator | Multiplication | Parameters: Factor 2.00 | Apply | OK).
- To remove clean tooth areas from the images, subtract the green channel image series from the enhanced red channel image series (Edit | Image calculator | Second operand images: Planimetry_green | Subtraction | Apply | OK).
- To identify the plaque-covered areas on the teeth, perform a threshold-based segmentation of the resulting image series (Segment | Automatic segmentation | Custom threshold). Set the "Low" threshold above the intensity of the clean tooth areas (i.e., 80). Leave the "High" threshold at 255. Only plaque-covered areas are recognized as objects in the software. Click on Apply | OK | Segment! to initiate the segmentation.
- Perform a visual quality control of the segmented images in the object editor, and delete artifacts by rejecting and deleting such objects. Merge the remaining objects in all the images (In all images | Merge selected objects). Quantify the plaque-covered area in each image (Analysis | Measure objects | Clear all | Pixels). Export the data.
- Open the exported data tables in a dedicated software. Calculate the PPI according to equation (1):
Equation (1)
The presented method allows for the rapid, semi-automated planimetric quantification of plaque-covered areas on teeth (Figure 1). Plaque deposits are visualized by erythrosine, while clean tooth areas as well as the acquired pellicle are left unstained16 (Figure 2A). When images are acquired with a fluorescence camera, the contrast between the clean tooth areas, plaque-covered areas, and surrounding soft tissues is enhanced considerably (Figure 2B,C). The fluorescence camera operates with two detection windows, one in the green and one in the red spectrum. Compared to the clean tooth areas, the plaque-covered areas appear slightly brighter in the red channel (Figure 2D,E). In the green channel, the autofluorescence of the tooth is masked considerably in the plaque-covered areas (Figure 2F). This masking effect is exploited during image analysis, when the green channel images are subtracted from the red channel images (Figure 2G). The strong contrast between the clean and plaque-covered areas in the resulting images (Figure 2H) allows for an intensity threshold-based, semi-automated determination of the PPI. Up to 1,000 fluorescence images can be processed simultaneously.
A custom-made 3D-printed spacer may be used to improve the standardized positioning of the camera head at an identical distance from the tooth of interest. The spacer also shields the tooth from ambient light and thereby enhances the contrast between the disclosed plaque, clean tooth areas, and surrounding soft tissues in the acquired images. The spacer is mounted on the camera head with the help of three retention elements (Figure 3).
The described method can be used for planimetric recordings of the supragingival plaque and calculus on both facial and oral tooth surfaces (Figure 4A–D). Depending on the curvature of the dental arch, it can be difficult to position the spacer in close contact with the gums and thereby keep the same distance between the camera head and the tooth. As the plaque area coverage is determined relative to the total tooth area, such differences are unlikely to affect the PPI recordings. Different tooth-colored materials fluoresce in the green spectrum with varying intensities17,18,19. Hence, the PPI can usually be determined with the standard image analysis algorithm on teeth with glass ionomer cements and composite resin restorations (Figure 4E–H). In contrast, amalgam and cast restorations usually emit faintly in both the red and the green channels, and it is, thus, not possible to determine the plaque coverage on such surfaces (Figure 4I,J). The same holds true for metallic orthodontic brackets, but since the bracket surface is typically excluded from PPI recordings, semi-automated planimetry is suitable for orthodontic patients (Figure 4K,L).
The successful semi-automated identification of plaque-covered areas on fluorescence images is highly dependent on the careful execution of all the steps of the clinical procedure. If too much ambient light enters the images, the brightness of the background in the red channel is increased, which renders the differentiation between the teeth and soft tissues difficult (Figure 5A,B). Therefore, the room lights need to be dimmed during the image capture. If the patient does not open the mouth sufficiently during the image acquisition, antagonist teeth may be imaged along with the tooth of interest and hamper the semi-automated processing (Figure 5C). When planimetry is performed on premolars or molars, the correct angulation of the camera is important to avoid imaging parts of the occlusal surface (Figure 5D,E). Once the plaque deposits are disclosed, the operator should immediately proceed to the image acquisition. Otherwise, the erythrosine may be washed out, and the contrast between the plaque-covered and clean tooth areas may become too faint. In some instances, however, the disclosing solution may strongly stain the gingiva, and the stain may not be removed during the following rinse (Figure 5F). To avoid an overestimation of the plaque-covered area, the stain may be reduced by an additional rinse or by gentle wiping of the gingiva with a cotton pellet.

Figure 1: Workflow for the semi-automated quantification of plaque coverage on tooth surfaces. Abbreviation: PPI = planimetric plaque index. Please click here to view a larger version of this figure.
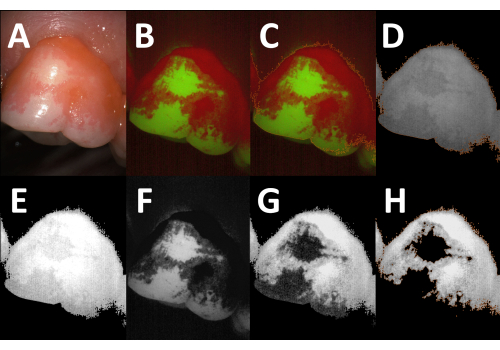
Figure 2: Digital image analysis procedure. (A) White-light image of disclosed plaque (tooth 26, facial aspect). (B) Corresponding image acquired with a fluorescence camera (Red-Green-Blue [RGB] mode). Note the enhanced contrast between the plaque-covered and clean tooth areas. (C) The total tooth area, marked by the orange outline, is identified by intensity threshold-based segmentation. (D) The object layer from the RGB image is transferred to the red channel image (orange outline), and the non-object pixels (background, soft tissues) are deleted. (E) The brightness of the red channel images is enhanced by a factor of two. (F) The green channel image. Note the reduced autofluorescence in the plaque-covered areas. (G) After subtraction of the green channel image (F) from the modified red channel image (E), the contrast between the plaque-covered areas and clean tooth areas is evident. (H) After intensity threshold-based segmentation, the plaque-covered areas are identified as objects (orange outline), and the planimetric plaque index (PPI) can be calculated (PPI = 81.6%). Please click here to view a larger version of this figure.

Figure 3: Custom-made spacer. A custom-made spacer viewed from the (A) front, (B) side, and (C) back. (D) Fluorescence camera with the mounted spacer (orange outline). Please click here to view a larger version of this figure.

Figure 4: Applications and limitations of semi-automated planimetry. (A) Fluorescence image of a facial tooth surface. (B) Corresponding processed image showing the plaque-covered areas (orange outline; planimetric plaque index [PPI] = 51.9%). (C) Fluorescence image of an oral tooth surface. (D) Corresponding processed image showing the plaque-covered areas (orange outline; PPI = 14.5%). (E–H) Images of teeth with composite resin restorations. The restoration in E fluoresces strongly in the green spectrum, whereas the restoration in G appears slightly fainter than the surrounding clean tooth areas. In both images, the PPI can be determined using the standard image analysis algorithm. (F,H) Processed images showing the plaque-covered areas (orange outlines; PPI = 20.3% and 20.2%, respectively). (I,J) Fluorescence images of a tooth with an amalgam restoration (I) and a tooth with a metal-ceramic crown (J, blue outline, added manually). Both restorations are non-fluorescent, and the plaque deposits cannot be quantified by semi-automated planimetry. (K) Fluorescence image of a tooth with a metallic orthodontic bracket. As the bracket is excluded from the analysis, the PPI can be determined using the standard image analysis algorithm (L, orange outline, PPI = 31.5%). Please click here to view a larger version of this figure.
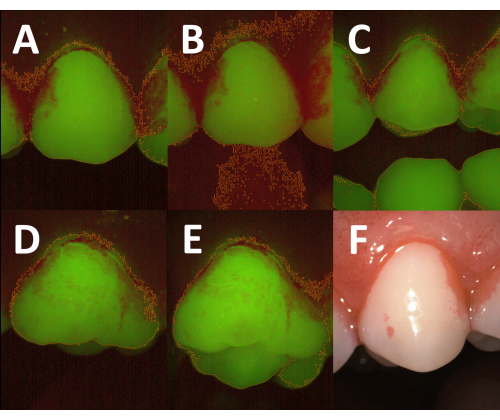
Figure 5: Influence of the clinical procedures on image quality and the results of semi-automated planimetry. (A) Fluorescence image acquired with dimmed room lights. The total tooth area is determined correctly after threshold-based image segmentation (orange outline). (B) Fluorescence image of the same tooth acquired with the room lights turned on. Due to an increased background emission in the red spectrum, the threshold-based segmentation fails to differentiate accurately between the tooth surfaces and the surrounding soft tissues (orange outline). (C) Fluorescence image acquired with insufficient mouth opening. The undisclosed antagonist teeth are visible in the image and, thus, included in the total tooth area (orange outlines). To obtain a correct planimetric plaque index, they have to be removed manually during the image analysis. (D) Fluorescence image acquired with optimal positioning of the camera head. The total tooth area (orange outline) is limited to the facial aspect. (E) Fluorescence image of the tooth in D acquired with suboptimal angulation of the camera head. Part of the occlusal surface is captured, resulting in an increased total tooth area (orange outline). (F) White-light image of disclosed plaque with prominent staining of the gingiva. The high emission in the red spectrum may lead to an overestimation of the plaque-covered area. Please click here to view a larger version of this figure.
Supplemental File S1: Please click here to download this File.
