Fonte: Joseph Donroe, MD, Medicina interna e pediatria, Yale School of Medicine, New Haven, CT
Mentre la sua utilità nello screening del cancro è dibattuto, l’esame rettale maschile rimane una parte importante dell’esame fisico. L’esame è indicato in pazienti selezionati con sintomi del tratto urinario inferiore, incontinenza o ritenzione urinaria e/o fecale, mal di schiena, sintomi anorettali, disturbi addominali, pazienti traumatizzati, anemia inspiegabile, perdita di peso o dolore osseo. Non ci sono controindicazioni assolute all’esame rettale; tuttavia, le controindicazioni relative includono la riluttanza del paziente a sottoporsi all’esame, grave dolore rettale, recente intervento chirurgico o trauma anorettale e neutropenia.
Quando si esegue l’esame rettale, l’esaminatore dovrebbe concettualizzare l’anatomia pertinente. Lo sfintere anale esterno è la parte più distale del canale anale, che si estende da tre a quattro centimetri prima di passare al retto. La ghiandola prostatica si trova anteriormente al retto, appena oltre il canale anale. La superficie posteriore della prostata, compreso l’apice, la base, i lobi laterali e il solco mediano, può essere palpata attraverso la parete rettale (Figura 1). La normale consistenza della prostata è simile all’eminenza thenar quando la mano è in un pugno stretto. La nocca del pollice è rappresentativa di come può essere un nodulo duro. La dimensione normale della prostata aumenta con l’età ed è di circa 4,0 cm per 3,5 cm, o 20-30 g, in un giovane.
Le fasi dell’esame rettale maschile, tra cui preparazione, posizionamento, valutazione neurologica, ispezione esterna e palpazione, esame della prostata e del retto e valutazione delle feci, sono dettagliate in questo video.
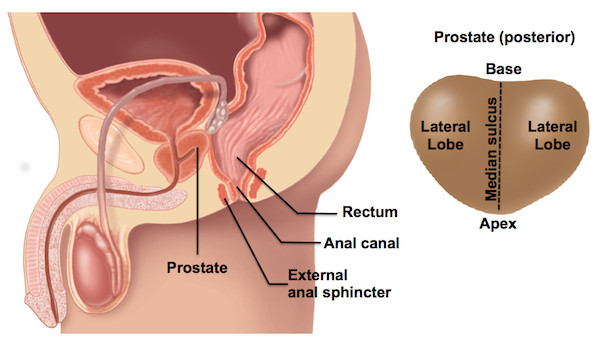
Figura 1. Anatomia rettale maschile (a sinistra) e regioni della superficie posteriore della ghiandola prostatica (destra).
The male rectal exam remains an important part of the physical exam, particularly for patients with abdominal, genitourinary, or gastrointestinal concerns. It is a sensitive procedure and requires careful attention to verbal and body language to ensure patient comfort. This video reviewed the indications and contraindications for the exam, relevant anatomy, as well the steps involved in performing the examination. Abnormalities that may be encountered at each step are found in Table 1. Physician comfort and technical proficiency with the rectal exam improves through practice, and the accuracy of the exam correlates with the experience of the examiner. As in other aspects of the physical exam, it is important to have a systematic method of examination. The method demonstrated in this video involves neurologic assessment, inspection and palpation of the perianal region, palpation of the prostate, palpation of the rectum, and finally, inspection of any stool on the gloved finger after the exam.

Table 1. Abnormalities detected during the male rectal exam. The table shows potential pathological findings that can be observed during rectal examination and their interpretations.
Limitations of the rectal exam are important to become familiar with. The rectum extends 12 to 15 cm beyond the anal canal, thus only the most distal portion can be palpated. Additionally, determining prostate size by DRE may be unreliable and thus should be considered an approximation. When compared with experienced urologists, students tend to palpate fewer areas of the prostate and use insufficient pressure, both of which limit detection of nodules. The examiner should always attempt to palpate the prostate from apex to base and both lateral lobes. However, with larger prostates, the examiner's finger may not be long enough to reach the base, limiting the evaluation. Finally, early malignancy is unlikely to be detected by DRE alone, thus screening for prostate cancer should be done with concomitant prostate specific antigen (PSA) testing in the appropriate patients.