The observation of spontaneous calcium oscillation in mNG-GECO10 expressed by iPSC-derived cardiomyocytes (iPSC-CMs) with or without drug treatments is demonstrated in Figure 1 and Animated Video 1. Kinetic traces obtained using mNG-GECO show that small molecular ion channel inhibitors, verapamil, dofetilide, and E4031, affected calcium transients (Figure 1B) as expected. The typical calcium transient shown in Figure 1C can be analyzed by Calcium peak analysis software to derive Peak signal (Amplitude), Calcium transient duration 50% (CTD50), Calcium transient duration 90% (CTD90), rise time, and decay time. Verapamil, an L-type calcium blocker17, completely inhibits the calcium influx in the cells as expected (Figure 1B). Dofetilide and E4031 are hERG channel inhibitors18,19,20, listed as experimental class III antiarrhythmic drugs. The decay time is prolonged with both Dofetilide (p < 0.05) and E4031 treatment (p < 0.001) when compared with the vehicle group. Prolongation of CTD50 (p < 0.01) and CTD90 (p < 0.001) with E4031 treatment was observed compared with vehicle only (Table 1), these results are consistent with reported effects on the QT interval, a clinically relevant measurement of repolarization determined from the surface electrocardiogram from a long time between the start of the Q-wave and the end of T-wave, in previous studies12,21.
A difficulty of CTD assessment in spontaneously beating cells is the variability beat rate imposes on the CTD. This is a particular problem for the iPSC-CM model, where each well of a 96 well plate can have its own beat rate even though all cells come from the same parent vial. It is possible to impose a beat rate by optical or electrical pacing. To evaluate the dose-response of E4031 under standardized paced conditions, ChR2 and K-GECO7 expressing iPSC-CMs were optical controlled using 1 Hz 470 nm pulses of light and observed using the red K-GECO signal (Figure 2A and Supplementary Figure 1). Progressive reductions of peak amplitude (p < 0.01) and increase in decay time (p < 0.05) of the calcium transients occur with increasing concentrations of E4031 (Figure 2B1). A dose-dependent effect of E4031 was most apparent for the reductions in peak amplitude (Figure 2B1,B2).
Although short-term studies lasting minutes are typically used for cardiotoxicity assessments, there is a blind spot for chronic toxicity assessments which parallel patient exposures to drugs over weeks, months, or years. It would be advantageous to study disease, or toxicity, effects over the intervals reflecting the treatment durations relevant to clinical practice. We utilized our all-optical control and detection system to study the iPSC-derived cardiomyocytes from a patient with left ventricular non-compaction (LVNC). iPSC-CMs were transduced with a K-GECO viral kit (step 2.2-2.6) post differentiation Day 25. The K-GECO signal was then tracked every 1-2 weeks in the same wells, with or without additional drug treatments. Both spontaneous calcium activity (Figure 3A,3B) and calcium dynamics under optical pacing (Figure 3C,D, step 4.11) were obtained using the high-Content Imaging System (step 4.1-4.12) and processed by calcium peak analysis software (step 6). As demonstrated in Figure 3A,C, clear calcium transients remain visible a month after viral transduction, with or without the additional light used for optical pacing. This work identified a drug that appears to increase beat rate, regularise contraction interval, and increase the transient calcium amplitude in the LVNC iPSC-CM model (Figure 3A,B). There are two important observations to make from this data. Firstly, from the therapeutic perspective, the drug effect appears durable at Day 63 and Day 70-time points. Secondly, and of relevance to a field which in general assays compound effects during brief windows (<1 min) at earlier time-points (typically <50 days); the disease phenotype modifying effects of the compound are only apparent after Day 60, suggesting it may be easy to discount drugs which have slow mechanisms of action in standard screening protocols.
The variability of beat frequency, and the subsequent impact on calcium transient duration, is not just a well-to-well problem at any given time point. It also changes as iPSC-CM are maintained in culture, which varies within a well over time (Figure 3B). To impose consistency within sequential experiments, 1 Hz optical pacing can be applied with or without drug treatment (Figure 3C,D). Here although the Day 63 results show the encouraging trends in the calcium transient with a significantly higher amplitude, shorter CTD90, and shorter decay time; by the 70 day time-point – and indicative of the need for chronic assessments during the drug screening process for rare disease – early after depolarizations (EAD) are detected. The value of adding a pacing protocol to disease phenotyping, or small molecule evaluation, can be qualitatively assessed by comparison of the results presented in Figure 3B,D for beat rate, calcium transient amplitude, CTD90, and decay time.
An advantage of a GECI, compared to chemical dye, based methodology to visualize the calcium transient is the ability to restrict the probe to a specific compartment within a cell. This can be further expanded by multiplexing multiple color and/or affinity variants in single cells. Hence, several GECIs including ER-LAR-GECO9, mtGCEPIA22,23 (or Oria1-G-GECO), and NIR-GECO28,24 have been developed for expression singly, or in combination, in cell models for real-time calcium activity measurement arising in the endoplasmic reticulum / sarcoplasmic reticulum (ER/SR), mitochondria (or CRAC channel) and cytosol, respectively. They can be combined in the iPSC-CM model (Figure 4A,C) to study the interaction between different intracellular calcium stores. For example, 10 mM caffeine treatment can be used to empty the SR calcium store. Here a decrease of ER-LAR-GECO signal (indicative of loss of calcium from the SR) paralleled a decline of the NIR-GECO signal (indicative of an increase in cytosolic calcium concentration) as expected. How other intracellular compartments are affected by these fluctuations is not well studied. Still, the inclusion of a green mitochondrial-targeted mtGCEPIA3 shows that calcium uptake occurs in mitochondria in these conditions (Figure 4A,B).
Similarly, visualizing the interplay between different calcium currents can be seen by including a probe, Orai1-G-GECO25, to reveal the calcium release-activated channel (CRAC) Ca2+ current (Figure 4C,D). In the iPSC-CM model, this signal increases with the spontaneous cytosolic calcium transient (Figure 4D1,D2). In keeping with this, treatment with caffeine evokes a large calcium transient in both the cytosol and from the Orai1 channel.
It is acknowledged that most calcium transient imaging in cardiomyocyte models has been determined using calcium dyes26. A genetically encoded calcium indicator was compared to a chemical dye in the iPSC-derived cardiomyocyte model to enable a side-by-side comparison of different calcium imaging approaches. K-GECO expressing iPSC-CMs were imaged alongside Fluo-4 loaded cells. K-GECO expressing cardiomyocytes showed consistent beating behavior over time (Figure 5A,C). However, Fluo-4 loading impacted both the beat frequency and CTD in this model (Figure 5B,C), suggesting Fluo-4 itself might influence the results of such experiments. This will be especially true after long-term exposure to the imaging probe, which can occur in the multiwall imaging format if well-by-well imaging occurs with a minute dwell time per well.
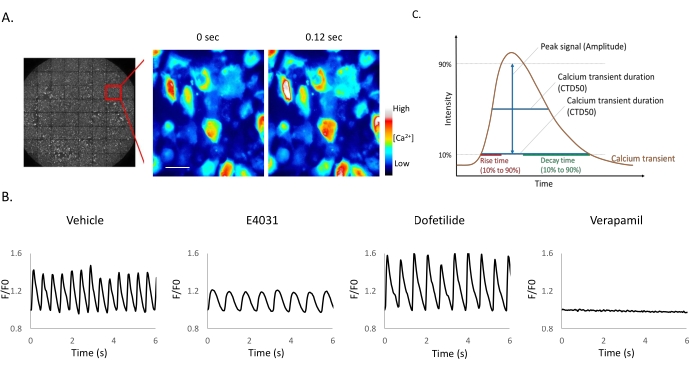
Figure 1: Small molecule ion channel inhibitors applied to iPSC-derived cardiomyocytes. (A-B) Time-lapse images of iPSC-CM expressing mNG-GECO taken at 25 Hz. Scale bar = 50 µm. (B) Representative Ca2+ oscillations after compound addition. Fluorescent signals obtained from mNG-GECO expressing cells are presented as a fluorescence ratio F/F0, where F0 is defined as basal intensity and F the intensity detected at each time point. (C) Calcium peak analysis software can extract parameters including half-maximal width (CTD50), 90% transient duration (CTD 90), rise time, and decay time. Please click here to view a larger version of this figure.

Figure 2: Dose-response example using the hERG inhibitor E4031 within an optical pacing system. (A) Traces of optical stimulation with 10% blue light in different concentrations of E4031. Time-lapse images of iPSC-derived cardiomyocytes expressing K-GECO taken at 25 Hz. (B1) Representative traces of calcium transients obtained with different compound doses. Peak analysis and dose-response of E4031 in amplitude (B2) and Decay time (B3). Blue bars indicate 1 Hz 470 nm pulse light stimulation. Please click here to view a larger version of this figure.
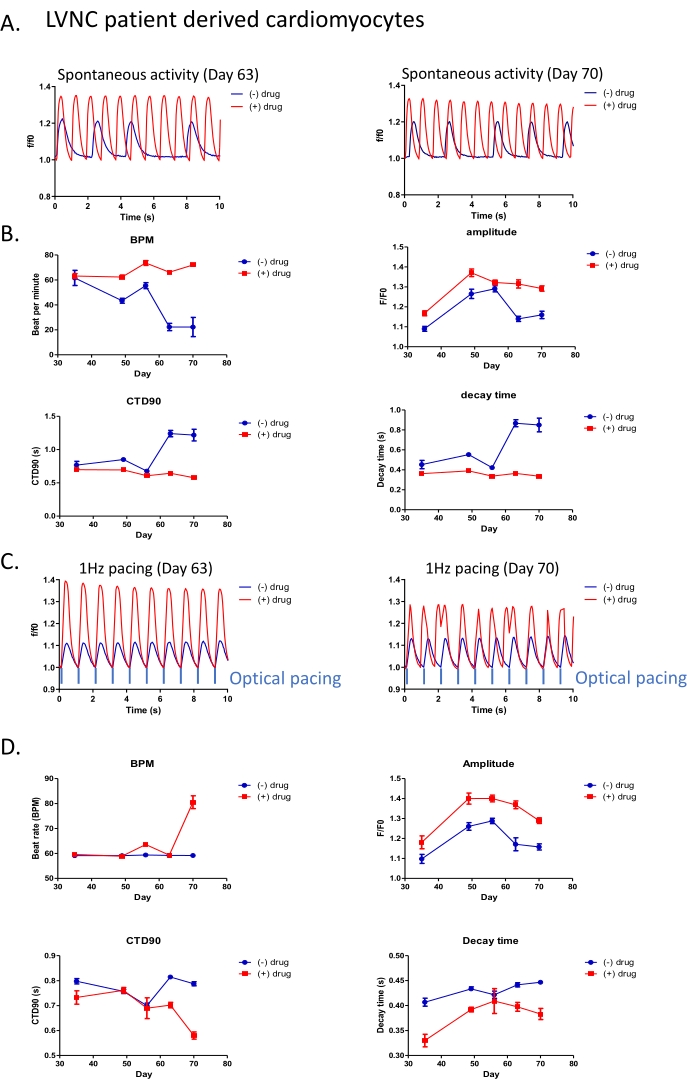
Figure 3: All-optical platform applied for long-term drug phenotypic screening in LVNC patient-derived cardiomyocytes. (A) Representative trace of spontaneous beating activity in patient-derived cardiomyocytes (post differentiation Day 70) with (red) or without (blue) 5 µM drug treatment. (B) Peak analysis of spontaneous beating activity with or without 5 µM drug treatment. (C) Intensity traces of drug response in patient-derived iPSC-CM under 1 Hz optical stimulation. (D) Peak analysis of patient-derived cardiomyocytes with 1 Hz optical stimulation. Please click here to view a larger version of this figure.
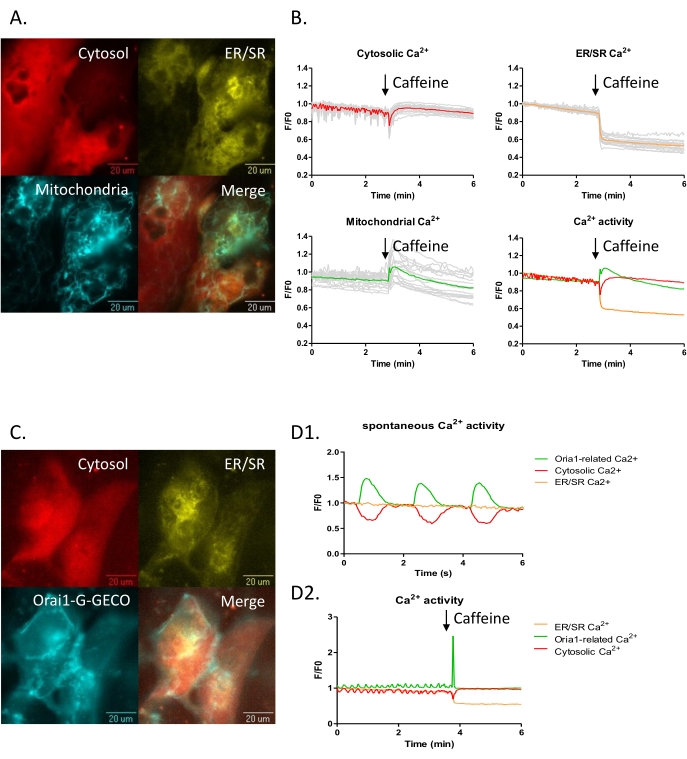
Figure 4: Three channels subcellular Ca2+ imaging in the iPSC-CM model. (A-B) iPSC-CMs were transduced with subcellular calcium probes for the cytoplasm, NIR-GECO2 (red), the endoplasmic reticulum ER-LAR-GECO (yellow), and mtGCEPIA3 (cyan), a mitochondrial Ca2+ indicator. (B) Three-channel time-lapse calcium imaging before and after 10 mM caffeine treatment. (C-D) iPSC-CMs transduced with cytoplasmic, NIR-GECO2 (red), endoplasmic reticulum ER-LAR-GECO (yellow), and CRAC channel indicators Orai1-G-GECO (cyan) were visualized. (D) Three-channel time-lapse calcium imaging was captured. (D1) Spontaneous beat-to-beat activity was observed with NIR-GECO2 and Orai1-G-GECO. (D2) Calcium efflux from the ER (decrease of ER-LAR-GECO signal) accompanied an increase in the cytosolic calcium signal upon caffeine treatment. Please click here to view a larger version of this figure.
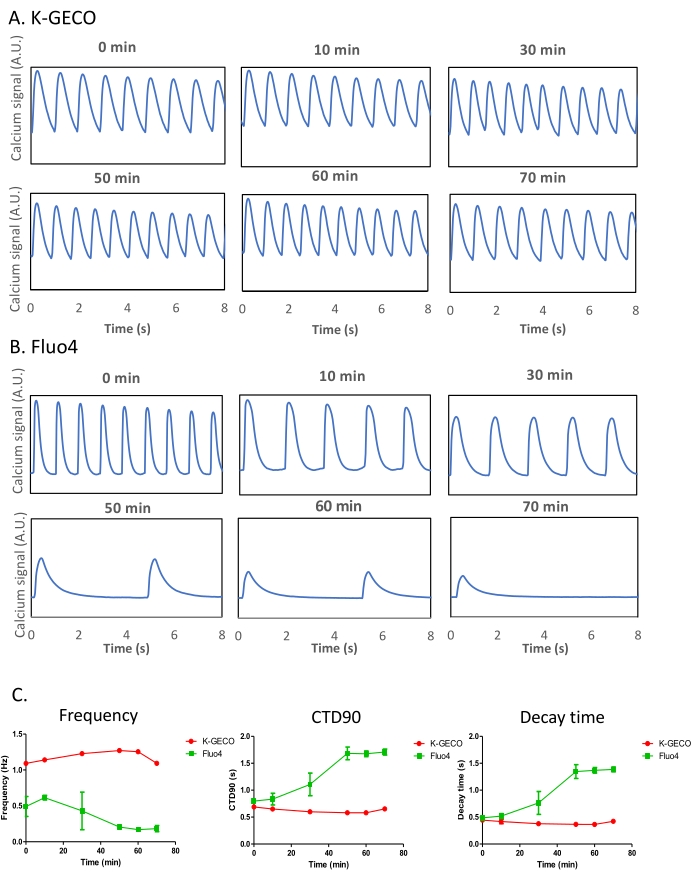
Figure 5: Comparison of the genetically encoded calcium indicator (K-GECO) to the chemical calcium-sensitive dye (Fluo-4) in iPSC-CMs. (A-B) Representative calcium traces of K-GECO (A) and Fluo-4 (B) are presented over time. (C) Calcium transient analysis of K-GECO transduced, or Fluo-4 loaded iPSC-CM. Please click here to view a larger version of this figure.
| BPM | CTD50 (s) | CTD90 (s) | Amplitude (F/F0) | Rise time | Decay time (s) | |
| Vehicle (0.1% DMSO) | 112.3657+/-10.95 | 0.25+/-0.04 | 0.41+/-0.01 | 1.99+/-0.02 | 0.07+/-0.01 | 0.28+/-0.01 |
| Verapamil (1 uM) | 0 | – | – | – | – | – |
| Dofetilide (5 nM) | 103.42+/-9.87** | 0.23+/-0.03 | 0.46+/-0.03 | 1.91+/-0.03 | 0.07+/-0.01 | 0.35+/-0.02* |
| E4031 (30 nM) | 75.73+/-12.08*** | 0.37+/-0.04** | 0.58+/-0.08*** | 1.55+/-0.02** | 0.11+/-0.04*** | 0.35+/-0.07** |
Table 1: Effects of compound addition to transient calcium parameters in the iPSC-CM model. Significance values are indicated by *(p ≤ 0.05), **(p < 0.01) and ***(p < 0.001).
Animated Video 1: Spontaneous calcium activity was observed by mNG-GECO in iPSC-derived cardiomyocytes with vehicle only. A Pseudo-coloured movie of a grey-scale image is provided. Please click here to download this Video.
Supplementary Figure 1: Schematic representation of the adenoviral-vector. This includes channel rhodopsin ChR2 as an actuator, with a red fluorescent calcium indicator K-GECO as a calcium reporter for an all-optical assay. The light-sensitive ion channel allows excitable cells to be depolarized by light in the blue-green range of the visible spectrum. 470 nm light was used in these experiments. Calcium transients in excitable cells can simultaneously be imaged by K-GECO, which requires green excitation light, producing red emissions. Please click here to download this File.
