An informed, written consent has been signed by all participants. This study was approved by the Ethics Committee of the University of Milan (n. 48/19) and conducted in accordance with the Declaration of Helsinki.
1. Training of experimenters
- Take the grating tool and apply a force of 100 g on a sponge placed on a scale.
NOTE: Refer to Figure 1 for the schematic of the grating tool used in this study - Repeat this procedure at least 10 times to reduce variation in the force applied by the grating on the subjects' tongues during testing, both within and across experimenters.
2. Assessment procedure
NOTE: Conduct the assessment of tactile acuity following the required health and safety standard to guarantee the subject's safety (e.g., mask, gloves, and lab coat).
- Display all gratings (0.20 mm, 0.25 mm, 0.50 mm, 0.75 mm, 1.00 mm, 1.25 mm) (Figure 2) on a table out of sight of the participant.
- Seat the participant in a comfortable chair and inform them that they can leave the experiment at any time.
- Inform the participant that they will be blindfolded during the experiment and asked to stick out their tongue in a comfortable and relaxed way.
- Prior to the beginning of the experiment, familiarize the subjects with the procedure using the largest grating (1.25 mm) to demonstrate the force applied (100 g for 3 s).
- Notify the participants that they can take a sip of water whenever deemed appropriate.
- Apply each grating onto the subjects' tongue (anterior region of the tongue just around the midline).
- After each touch, ask the subjects to indicate, using their hands, the tool's orientation (either horizontal or vertical) and their degree of sureness (sure, unsure). Subjects must guess if they do not know.
- After each touch, record all the answers (horizontal, vertical, sure, not sure) for each subject on a spreadsheet (Supplemental Table 1).
- Repeat each grating as many times as deemed necessary for the R-Index cut-off selected, for instance, 6 times, 3 horizontally, and 3 vertically (Supplemental Table 1).
- Sterilize each grating after testing each participant (refer to section 4).
NOTE: The tongue should protrude gently from the mouth without effort by the volunteers to avoid excessive fatigue, which would lead to an alteration in their performance results. It is important to note that the higher the repetitions by grating, the more reliable the measurement16.
3. Cleaning protocol
- Prepare a solution consisting of 20 mL of sodium hypochlorite (see Table of Materials) diluted in 1 L of water according to the manufacturer's instructions.
- Manually shake the solution for a few seconds.
- Fill 6 cups with approximately 20 mL of the disinfectant solution to fully immerse each tool in the solution.
- Place each tool in the corresponding cup.
- Let the tools soak for 15-20 min.
- Rinse the tools with plenty of water according to the manufacturer's instructions and scrub them with a toothbrush to ensure removing any sodium hypochlorite residue.
- Allow the tools to air dry.
4. R-index calculation
- Create a response matrix for each volunteer and for all the tools (Figure 3) based on the response frequencies used to calculate the R-index using the following equation:

NOTE: R-index expresses individual tactile sensitivity for each tool16. R- index is based on SDT17 and represents an estimated probability of discerning a target stimulus (i.e., the signal) from an alternative stimulus (i.e., the noise). The signal and the noise correspond to the correct or incorrect identification of the horizontal-vertical orientation of the grating. Four response options for both signal and noise can occur: "horizontal-sure", "horizontal-unsure", "vertical-unsure" and "vertical-sure"16. R-index values range between 0-1. A higher R-index value indicates better discrimination.
5. Sensitivity and threshold determination by the R-index estimates
- To determine whether a subject can discriminate the orientation of each tool, calculate the cut-off using a table of critical values for R-index significance tests18
NOTE: Considering the present example, corresponding to 36 presentations (i.e., each grating presented 6 times, 3 horizontal and 3 vertical), the cut-off value for discrimination is set to 0.7426 according to the one-sided R-index critical values for α = 0.0518. - If a sufficiently high number of tools is used (e.g., six different grating dimensions)19, derive R-index threshold estimations.
- To calculate the threshold for each subject, interpolate the two R-indices immediately below and above of the cut-off value20.
A total of 70 healthy adults (age range = 19-33 years; mean age = 22.0; 52.9% women) were involved in the study, as shown in Appiani et al. (2020)21.
As an example, the R-index distribution by age for square 0.75 mm is reported in Figure 4. Each point represents a different subject. Subjects above the dotted line (cut-off value: 0.7426) are those who correctly identify the orientation of the grating (more sensitive).
The performance for the six gratings and the derived R-index threshold estimate of one subject is reported in Figure 5. In this case, the threshold corresponds to 0.99 mm. Subjects with low threshold values are able to recognize a smaller bar size (more sensitive), while subjects with high threshold values require more input (larger bar size) to perceive the stimulus cognitively (less sensitive)10. In the present case, threshold values can range from 0.20-1.25 mm. Nevertheless, two extreme values can be achieved: subjects with a threshold <0.20 mm are those able to recognize the orientation of the squares from the smallest size (0.20 mm). Conversely, those participants who record a threshold >1.25 mm are unable to discriminate any of the grating sizes. An example of a threshold dataset is reported in Supplemental Table 2.
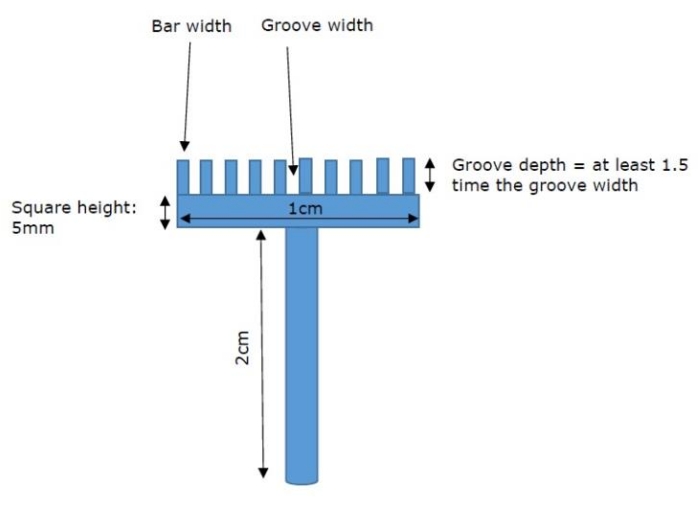
Figure 1: Description of the tools. Square schematic drawing Please click here to view a larger version of this figure.
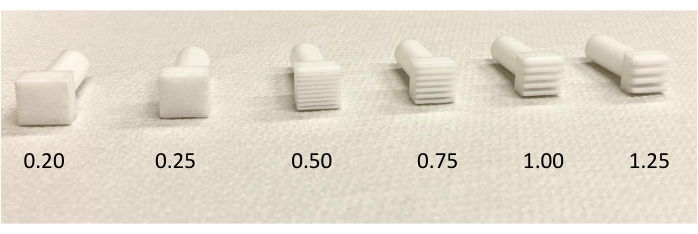
Figure 2: Squares with increasing-sized grooves/bars. The figure shows the six gratings, ranging from the smallest (0.20 mm) to the largest (1.25 mm). Please click here to view a larger version of this figure.
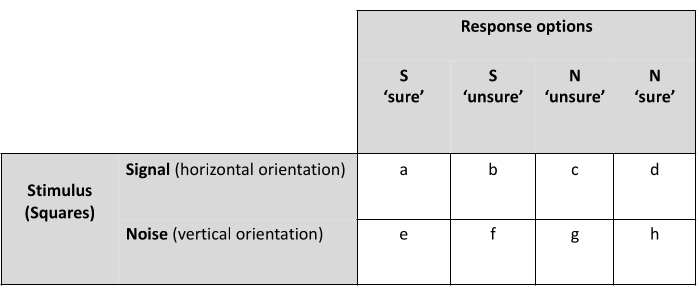
Figure 3: Response matrix. The figure shows the response matrix used to calculate the R index. Signal (S) and noise (N) correspond to the horizontal and vertical orientation, respectively. Letter from "a" to "h" are integers taking values between 0 and 3. Please click here to view a larger version of this figure.
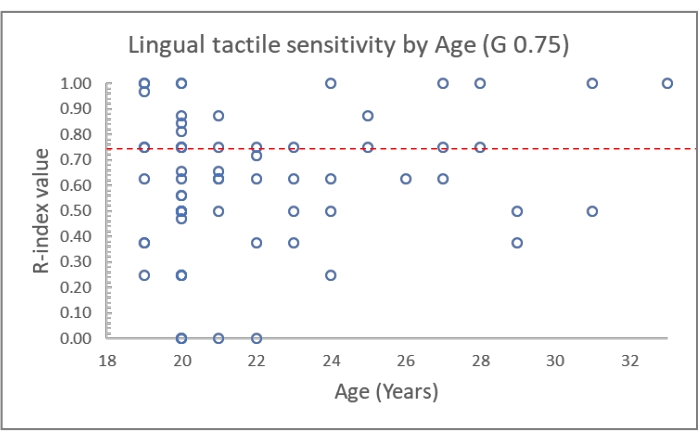
Figure 4: R-index distribution by age for square 0.75 mm. The dotted line represents the cut-off value (0.7426). Subjects that are above the dotted line are those that correctly identify the orientation of the tool. Please click here to view a larger version of this figure.
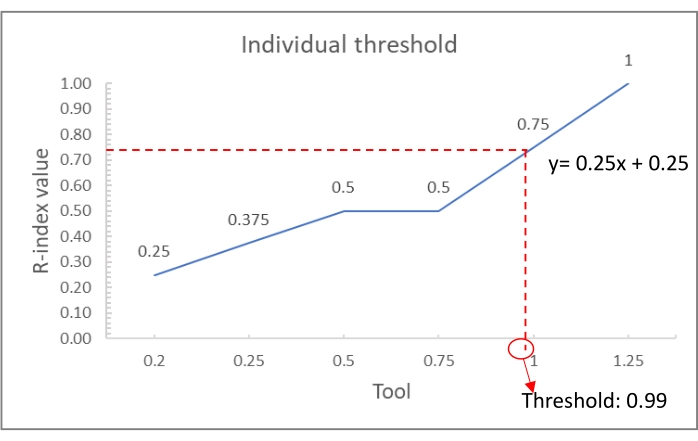
Figure 5: Individual threshold calculation. R-index values of one subject and calculation of the relevant threshold. Please click here to view a larger version of this figure.
Supplemental Table 1: An example of a spreadsheet used by the experimenters to record the participants' responses. The first column (Trial No.) represents the number of presentations; as an example, 36 possible presentations are reported. The second column (combination) indicates the size of the grating (G) and the orientation (HORIZ./VERT.). The investigator reports the subject's answer in the column "Answer" (Horizontal/Vertical) and indicates the degree of sureness using the last column (Sure/Unsure). Please click here to download this Table.
Supplemental Table 2: The dataset used to calculate individual thresholds. The first three columns report the identification code, the age, and the gender for each subject. Columns 4-9 report the R-index values for each tool. In bold are reported the values immediately above and below the cut-off that have been used for the calculation of individual thresholds through interpolation (last column). Please click here to download this Table.
