Common Magnetoencephalography signals
Common MEG signals are displayed in Figure 1, including a normal MEG signal (Figure 1A), as well as MEG signal noise due to metal on the participant (Figure 1B), in which case unlock the sensors, open the MSR door and ask the participant to remove any metal from their body, then take the metal object out of the MSR and perform an auto-tune before repeating the procedures outlined in section 3.5; interference from an electronic device (Figure 1C, most often from a mobile phone), in which case turn off any electronic devices or move them away from the MSR; a clenched jaw (Figure 1D), in which case remind the participant to relax their jaw for the duration of the MEG recording; alpha waves (Figure 1E; these are defined by eight to 12 continuous waves in a 1 s interval), in which case check that the participant is not asleep (it is fine to continue if they are awake); and trapped magnetic flux (Figure 1F); in which case unlock the sensors and turn on the coil heaters on for 5 min. If the flux persists after a subsequent auto-tuning, mark affected channel for removal from subsequent data analysis.
Head movement during data acquisition
Pediatric MEG data before and after ReTHM correction is displayed in Figure 2. Data was collected from a three-year-old boy who passively listened to auditory tones for 15 min. Data was de-noised10, band-pass filtered11 (1-15 Hz), baseline-corrected and averaged. Root-mean-square (RMS) magnetic waveforms (in the right column) were computed from all sensors. Averaged in-scanner head movements were 44.3 mm. As demonstrated, ReTHM compensated for motion-related artefacts, resulting in more focal isofield contour maps (at the peak of the RMS waveforms; (A), less distorted RMS magnetic waveforms (B), and more meaningful source reconstruction (C) in the bilateral auditory lobes.
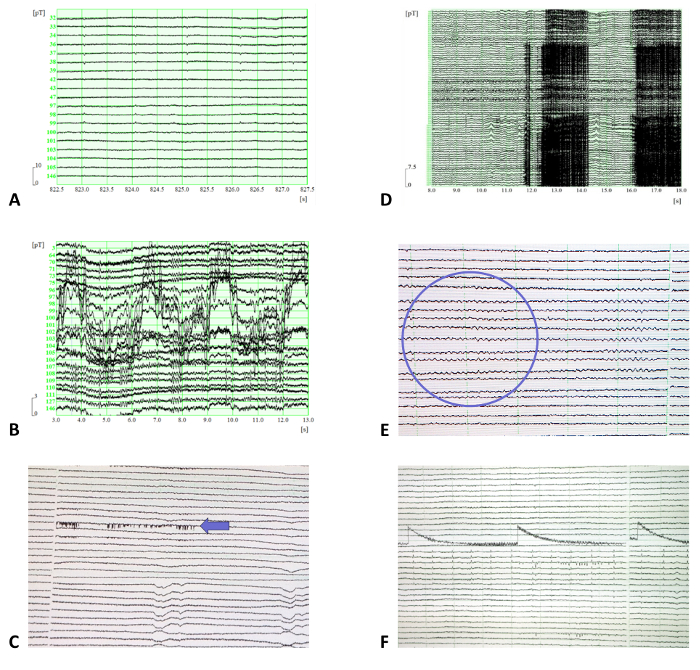
Figure 1: Examples of common MEG signals. (A) A normal MEG signal. (B-F) MEG signal noise due to (B) metal on the participant (specifically, noise caused by a small metal buckle on a singlet strap), (C) interference from an electronic device, (D) a clenched jaw, (E) alpha waves, and (F) trapped magnetic flux. For panels C, E, and F, the time scale on the x-axis is in 10-second intervals, and amplitude scale on the y-axis is 32768 A/D. Please click here to view a larger version of this figure.
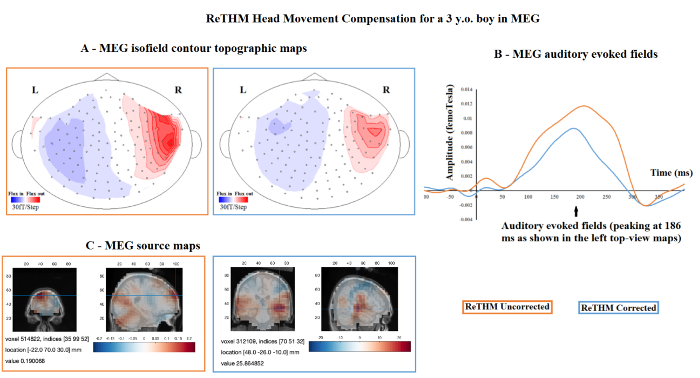
Figure 2. Pediatric MEG data before and after Real-Time Head Movement (ReTHM) correction. Data was collected from a three-year-old boy who passively listened to auditory tones for 15 min. Averaged in-scanner head movements were 44.3 mm. (A) More focused isofield contour maps at the peak of the root mean square (RMS) waveforms; (B) less distorted RMS magnetic waveforms, and (C) more meaningful source reconstruction in the bilateral auditory lobes are revealed after ReTHM correction. Please click here to view a larger version of this figure.
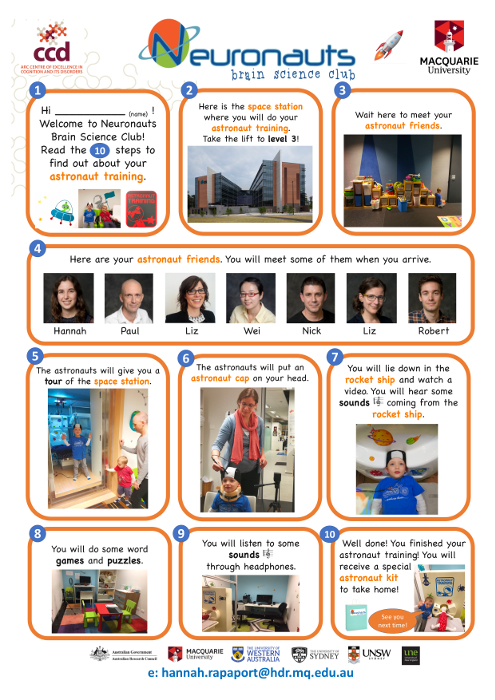
Supplementary Figure 1: A story board outlining 10 simple steps for completing the "astronaut training" (i.e., the MEG experiment). This is sent to families prior to visiting the MEG laboratory in order to guide children's expectations for the acquisition session, as well as to build excitement in anticipation of the "astronaut training". On data acquisition day, the children follow the story as the experiment progresses and collect stamps after completing each step. Photographs reproduced with informed written parental consent. Please click here to view a larger version of this figure.
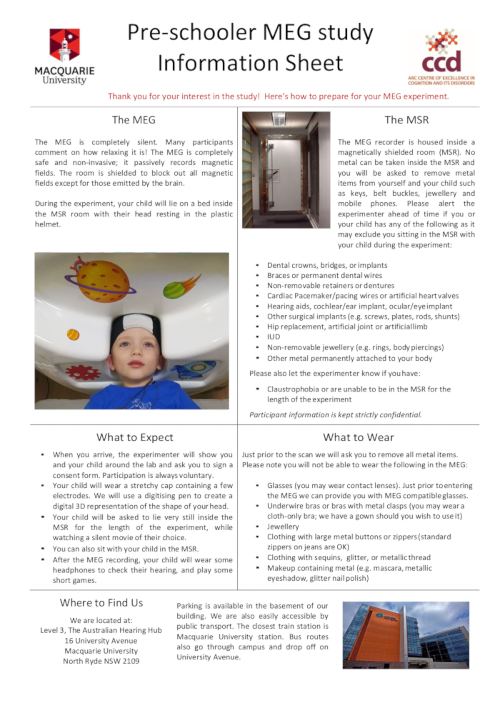
Supplementary Figure 2: An MEG information sheet for parents or caregivers explaining the MEG, the MSR, what to expect on data acquisition day and what to wear. Photograph reproduced with informed written parental consent. Please click here to view a larger version of this figure.
