The 3-step protocol for decellularization of human myocardium presented here results in near-complete removal of cellular material, while preserving the key ECM components and the fibrillar structure of ECM. After decellularization, the gross removal of cells from the tissue is evident by the change in color (Figure 1A). Histological analysis with H&E and Masson Trichrome stains revealed the complete absence of residual intact cells (Figure 1B). Quantitative assays for individual ECM components revealed a more complete DNA removal and better preservation of total collagen, elastin, and glycosaminoglycans as compared with decellularization by SDS alone (Figure 2A). Functional evidence of the biologic activity of cECM is shown in Figure 2B. Here, RT-PCR was used to quantify the expression of structural cardiomyocyte proteins (Myh6, Tnnt2), early (Mef2c, Nkx2.5) and late (Gata4) cardiomyogenic transcription factors, and endothelial cell surface marker genes (von Willibrand Factor (vWF), VE-cadherin) in murine ESC undergoing spontaneous differentiation. Compared to both uncoated culture dish surface and Matrigel-ECM coating, it is evident that contact with cECM drives pluripotent stem cells preferably towards a cardiomyocyte-like phenotype.
Lyophilized ECM slices can be further processed into microparticles without using enzymatic or chemical reagents. Mechanical grinding or pulverizing using suitable kits allowed for production of microparticles with a uniform size (Figure 3A). Mass spectrometry provides an overview of all recognizable proteins present in cECM. Gene ontology analysis concentrating on cellular components revealed that the majority of ECM proteins are indeed derived from extracellular space, with few hemoglobin residues and a number of predominantly intracellular proteins (Figure 4). This pattern may determine the tissue-specific biologic function of cECM, but this hypothesis needs further research. A summary of the cECM protein composition is shown in Table 1. Processing the ECM into microparticles preserves its biological activity. HL-1 cells exposed to simulated "ischemic" conditions (hypoxia, glucose and serum deprivation) displayed an increase in cell metabolism (Figure 3B) and a decrease in cell death when cultured on cECM (Figure 3C).
Limited pepsin-based digestion of the cECM powder, based on a modified protocol developed for collagen purification19, results in a homogenized ECM solution. Phase contrast light microscopy pictures (Figure 5A) demonstrate the digestion process after 0 h and 48 h. This homogenizing step facilitates applications in regenerative medicine10. The resulting processed cECM is shown in Figure 5B. Below room temperature it remains liquid (Figure 5B, left) but at 37 °C it forms a self-assembling hydrogel with stability suitable for an overlay with cell suspensions allowing 3D culture (representative picture, Figure 5B right, hydrogel layered with culture medium). Live/dead staining of human cardiac fibroblasts also shows the beneficial effects of culturing on cECM (Figure 5C). Both cECM microparticles and cECM hydrogel enhanced the metabolic activity of contractile HL1 cells in ischemic conditions as compared to cells in standard culture (Figure 5C, lower right panel).
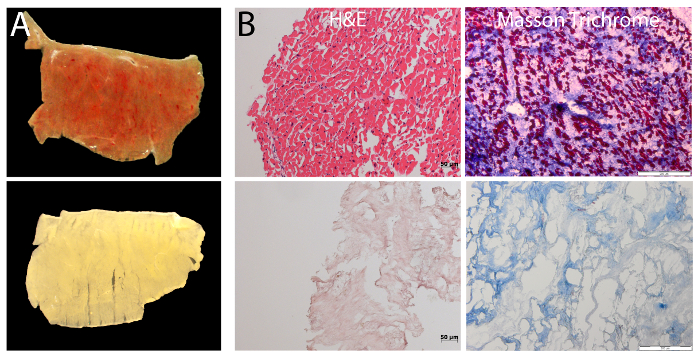
Figure 1: Decellularization of human cardiac myocardium. (A) Macroscopic analysis of cECM by stereo microscopy reveals the removal of cellular material with the 3-step decellularization protocol. This is evident by the increase in transparency. (B) Histology staining of myocardial slices before and after decellularization with HE- (left; Scale bar = 50 µm) and Masson Trichrome staining (right; Scale bar = 200 µm) shows successful removal of cells from the tissue. Please click here to view a larger version of this figure.
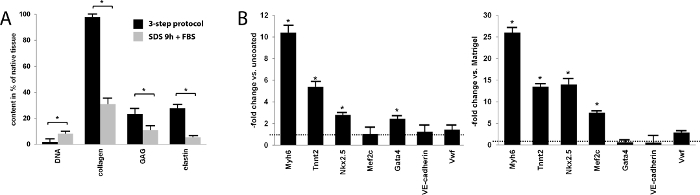
Figure 2: Content and effect of cECM slices. (A) Quantitative biochemical analysis of selected ECM components and DNA, comparing the 3-step decellularization protocol to 0.5% SDS-alone decellularization. Data are expressed as percentage of the content in native myocardium. With the 3-step protocol, the residual DNA content was nearly zero and significantly lower than that after a 9 h incubation with a standard combined 0.5% SDS/lysis buffer combination and FBS (SDS 9 h + FBS). Respective biochemical assays demonstrated a near-complete preservation of collagen, approximately 20% preservation of glycosaminoglycan content compared to native tissue, and a nearly 30% preservation of elastin content, all significantly higher than with the standard SDS reference protocol (Bars represent mean ± SEM). (B) mRNA expression of selected genes in induced pluripotent stem cells differentiating on cECM, compared to uncoated culture dishes and to Matrigel-coated surface. cECM data are normalized to those obtained on the respective control materials (control = 1, dashed line). The majority of cardiac genes are significantly more highly expressed when cultured on cECM (Bars represent mean ± SEM). Please click here to view a larger version of this figure.
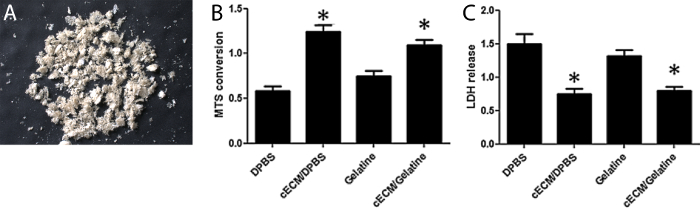
Figure 3: Appearance and biological activity of cECM microparticles. (A) cECM microparticle powder after lyophilization. (B) Metabolism (MTS) and (C) Cell death (LDH release) analysis of HL-1 cells cultured with cECM or gelatin. cECM significantly reduces cell death and increases metabolism. Bars represent mean ± SEM, statistical significance tested by one-way ANOVA and Bonferroni. Figure 3B-C have been modified from Kappler et al.18 Please click here to view a larger version of this figure.
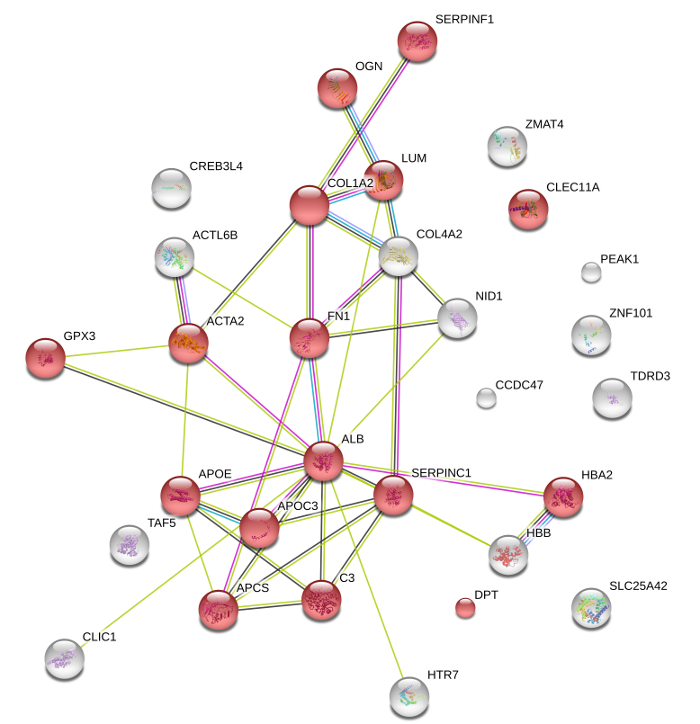
Figure 4: Protein composition of cECM microparticles. Following mass spectrometry, String DB analysis depicts the key components of cECM, which are mainly associated with the extracellular space (GO:0005615; red spheres p >0.05). Lines indicate protein interactions based on experimental-biochemical data (purple), on co-expression data (black), on database interactions (blue), and on co-expression (green). String DB required confidence: score >0.4. Please click here to view a larger version of this figure.
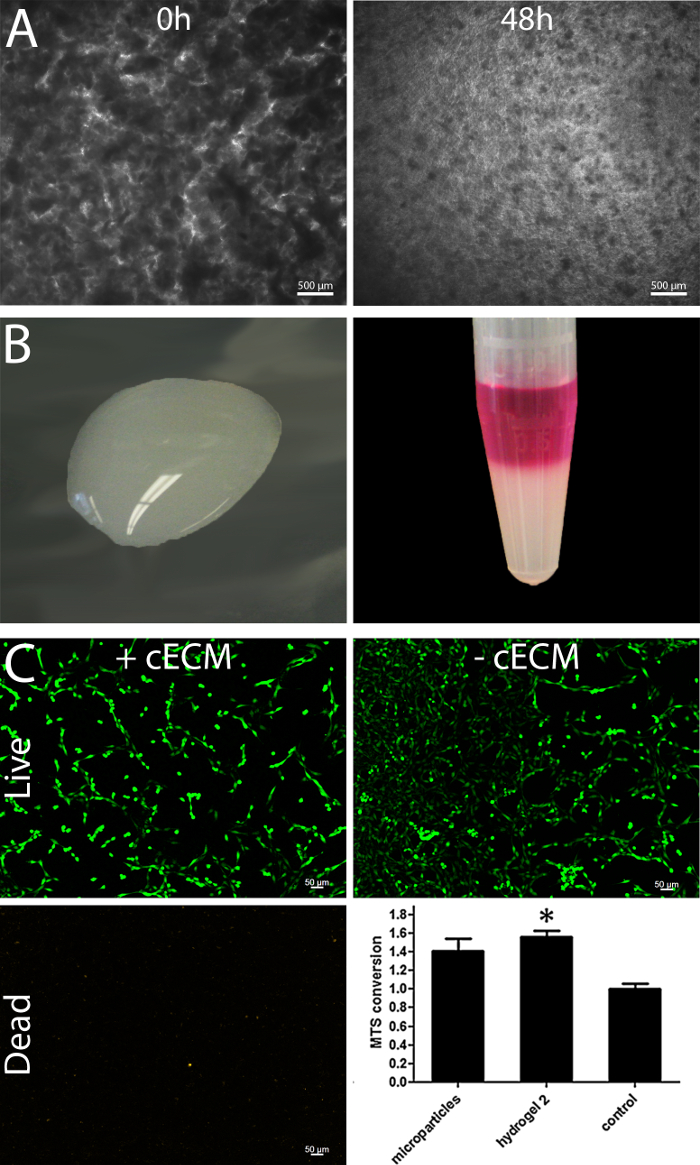
Figure 5: Processing of cECM to a hydrogel preserve the biological effectivity. Phase contrast light microscopy pictures demonstrate that enzymatic digestion of the cECM for 48 h results in a more homogenized ECM solution; Scale bar = 500 µm. (A) The ECM solution remains liquid up to room temperature (B, left) and contains the potential to self-assemble towards a hydrogel when incubated at 37 °C (B, right). Live/dead stain of cardiac human fibroblasts cultured with and without cECM reveals a higher calcein staining intensity of living cells; Scale bar = 50 µm (C). The cECM hydrogel increases the metabolic activity of HL1 cells in ischemic conditions in the same manner as the micro particles (C, lower right panel, modified from Kappler et al.18) Bars represent mean ± SEM, statistical significance tested by one-way ANOVA and Bonferroni. Please click here to view a larger version of this figure.
| Protein Description |
| 5-hydroxytryptamine receptor 7 OS=Homo sapiens GN=HTR7 PE=1 SV=2 |
| Actin-like protein 6B OS=Homo sapiens GN=ACTL6B PE=1 SV=1 |
| Actin, aortic smooth muscle OS=Homo sapiens GN=ACTA2 PE=1 SV=1 |
| Serum albumin OS=Homo sapiens GN=ALB PE=1 SV=2 |
| Antithrombin-III OS=Homo sapiens GN=SERPINC1 PE=1 SV=1 |
| Apolipoprotein C-III OS=Homo sapiens GN=APOC3 PE=1 SV=1 |
| Apolipoprotein E OS=Homo sapiens GN=APOE PE=1 SV=1 |
| Coiled-coil domain-containing protein 47 OS=Homo sapiens GN=CCDC47 PE=1 SV=1 |
| C-type lectin domain family 11 member A OS=Homo sapiens GN=CLEC11A PE=1 SV=1 |
| Chloride intracellular channel protein 1 OS=Homo sapiens GN=CLIC1 PE=1 SV=4 |
| Collagen alpha-2(I) chain OS=Homo sapiens GN=COL1A2 PE=1 SV=7 |
| Complement C3 OS=Homo sapiens GN=C3 PE=1 SV=2 |
| Collagen alpha-2(IV) chain OS=Homo sapiens GN=COL4A2 PE=1 SV=4 |
| Cyclic AMP-responsive element-binding protein 3-like protein 4 OS=Homo sapiens GN=CREB3L4 PE=1 SV=1 |
| Dermatopontin OS=Homo sapiens GN=DPT PE=2 SV=2 |
| Fibronectin OS=Homo sapiens GN=FN1 PE=1 SV=4 |
| Glutathione peroxidase 3 OS=Homo sapiens GN=GPX3 PE=1 SV=2 |
| Hemoglobin subunit alpha OS=Homo sapiens GN=HBA1 PE=1 SV=2 |
| Hemoglobin subunit beta OS=Homo sapiens GN=HBB PE=1 SV=2 |
| Ig kappa chain C region OS=Homo sapiens GN=IGKC PE=1 SV=1 |
| Lumican OS=Homo sapiens GN=LUM PE=1 SV=2 |
| Mimecan OS=Homo sapiens GN=OGN PE=1 SV=1 |
| Nidogen-1 OS=Homo sapiens GN=NID1 PE=1 SV=3 |
| Pseudopodium-enriched atypical kinase 1 OS=Homo sapiens GN=PEAK1 PE=1 SV=4 |
| Pigment epithelium-derived factor OS=Homo sapiens GN=SERPINF1 PE=1 SV=4 |
| Mitochondrial coenzyme A transporter SLC25A42 OS=Homo sapiens GN=SLC25A42 PE=2 SV=2 |
| Serum amyloid P-component OS=Homo sapiens GN=APCS PE=1 SV=2 |
| Transcription initiation factor TFIID subunit 5 OS=Homo sapiens GN=TAF5 PE=1 SV=3 |
| Tudor domain-containing protein 3 OS=Homo sapiens GN=TDRD3 PE=1 SV=1 |
| Zinc finger matrin-type protein 4 OS=Homo sapiens GN=ZMAT4 PE=2 SV=1 |
| Zinc finger protein 101 OS=Homo sapiens GN=ZNF101 PE=2 SV=1 |
Table 1: Protein composition of cECM powder as determined by mass spectrometry.
