Microenvironment/personal air sampling methodologies:
Figure 1Ai shows a pregnant mother wearing the customized vest during the 24 h sampling period. The vest includes the ECM, CO logger, and time and location logger with the power bank. It was ensured that the participants wore the vest throughout the sampling period, except while bathing and sleeping. The stand that was provided to hang the vest within the sleeping periphery is shown in Figure 1Aii.
Figure 1Bi shows cleaning of the ECM sampler during the pre- and post-sampling period and Figure 1Bii shows the calibration of ECM in the field laboratory. The flow rates were checked and the sampling runtime was set prior to sampling, and any deviations were checked in the post-sampling period.
Figure 1C shows the instrument placement (ECM, CO logger, and TLL) in the kitchen (1.5 m height from the ground) for area monitoring. The instruments were placed and installed 1 m away from the cooking source. When windows or doors were near the sources, the instruments were installed 1 m away from these openings. Figure 1D shows the instruments (ECM, CO logger, and TLL) connected with a power bank, installed (1.5 m height from the ground) outdoors in each participants' house. The results of microenvironmental and personal PM2.5 following these methodologies are already published24,35,36.
The data of CO logger calibration over 1 year showed low malfunctions, as shown in Supplementary Figure 8 (legend shown as a circle represents the measurement of the CO data logger reads beyond the calibration range of 0-50 ppm)35. Details about the difference between the blank and sample slot of BC measurement for loading the filter is given in the supplementary material (Annexure C).
Figure 1Ei illustrates damaged filters before the pre-weighing process. Damaged and dropped filters are flagged as invalid. Filters were rechecked at the field laboratory before loading into any air monitoring instruments. Similarly, sampled filters were examined for any damage, such as holes, tears, stretching, or dislodgment, as given in Figure 1Eii. If any such damage existed, it was weighed, but not considered as valid for subsequent analyses. PM2.5 mass for each sample was obtained by subtracting the sample mass from the median field blank mass. The final PM2.5 concentration was estimated by dividing the blank corrected filter masses by the amount of air sampled by the pump during the measurement interval. The derived threshold criteria for valid PM2.5 and CO sampling is given in Table 1. Data within the threshold criteria are considered valid and taken up for the analysis.
Stove use monitoring
Figure 3A shows the calibration of temperature loggers, which was done initially on ice and then in hot water with the help of a standard temperature monitor. Figure 3Bi shows the regular pattern of peaks which are considered valid and identified by characteristic peak color (orange) when the stove is used. As shown in Figure 3B, the irregular pattern of peaks, such as (ii) probe problem (recording high temperatures and measuring beyond the temperature range), (iii) technical error (baseline shift with negative values), and (iv) thermocouple problem, was characterized as invalid sampling (no records of temperature measurement; baseline shift together with negative values). The temperature logger installed in different cookstoves is illustrated in Supplementary Figure 5. The results of stove use monitoring following this methodology is already published18,19,36.
Ambient air sampling
With US EPA guidelines (https://www.epa.gov/environmental-topics/air-topics), the ambient samplers were installed at the top of one of the selected households in each representative HAPIN-India site (Figure 4A). Sampling sites were chosen based on security, availability of electricity, and willingness of the participant to host the monitor. Sites were selected to be in central areas relative to clusters of participants. Ambient samples followed a similar procedure of packing and shipping from the field site to the field laboratory to the central laboratory. To prevent cables from being plugged into the incorrect connector, connect with the unique pin layout as given in Supplementary figure 9. The results of ambient monitoring (PM2.5) measured between 2018 to 2020 is shown in Figure 4B. Also, the results of ambient monitoring using this method elsewhere is already published29.
Biomonitoring
Figure 5A displays the urine aliquoting procedure. The samples from the field site were stored in vaccine cooler bags and transported to the field laboratory, where they were aliquoted and stored in a deep freezer (-20 °C). Figure 5B summarizes the sample collection, transport, and field storage COC.
Figure 5C shows the DBSs; 5Ci shows valid spots before drying, and 5Cii shows valid spots after drying. Table 2 summarizes the pattern of valid DBS collection in follow-up visits among the HAPIN participants (M, OAW, C). The success rate of collecting valid DBSs from mothers for three visits is 100% (BL), 93% (P1), and 83% (P2). Similarly, for OAW, the success of DBS collection was consistent (100%-72%) for the first three (BL-P2) visits, but reduced (45%-35%) from B1 to B4 during the pandemic and during hurricane Gaja (2018). The success of DBS collection in children was 72.09% at birth (B0), 64% at B1, 62% at B2, and 45% at B4.
Figure 5D emphasizes that the cold chain with dry ice maintains sample integrity. Every month, biological samples were packed with dry ice in a separate thermal insulation box and shipped with temperature and relative humidity (RH) loggers. Correlation analysis of urinary specific gravity measured between the field laboratory and central laboratory showed good agreement, as shown in Figure 5E. Our results of biomonitoring method cross-validation in urine samples of polycyclic aromatic hydrocarbon metabolites shows the quality assurance (QA)/quality control (QC) of sample integrity21.
All sampling and CRF data were securely uploaded from SRIHER to Emory University's server. Data transfer occurred daily, thus reducing the likelihood of data loss. The list of CRFs used for data collection are given in Supplementary Table 3. The data collection flow from the field site to the Emory server is given in Supplementary Figure 10.

Figure 1: Personal and microenvironmental monitoring. (A) i) Pregnant mother wearing the vest with air sampling instruments (ECM, CO logger, and TLL); ii) Metallic stand with the vest; iii) Child vest with TLM units. (B) i) ECM cleaning; ii) ECM calibration. (C) Kitchen area monitoring with the ECM, CO logger, and TLL. (D) Outdoor area monitoring with the ECM, CO logger and TLL. (E) i) Damaged pre-weighed filters; ii) Damaged sampled filters. Please click here to view a larger version of this figure.
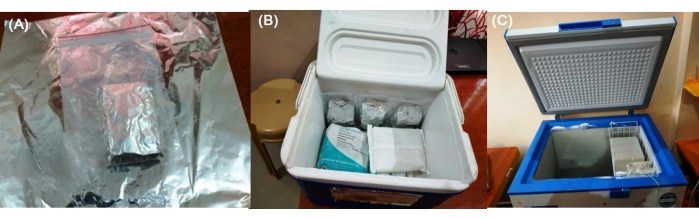
Figure 2: Chain-of-custody of filters. (A) Sampled ECM with filters wrapped up in aluminium foil. (B) Transport of sampled filters from participant households to the field lab in vaccine cooler bags containing gel packs. (C) Sample filters stored in a deep freezer (-20 °C) in the field laboratory. Please click here to view a larger version of this figure.
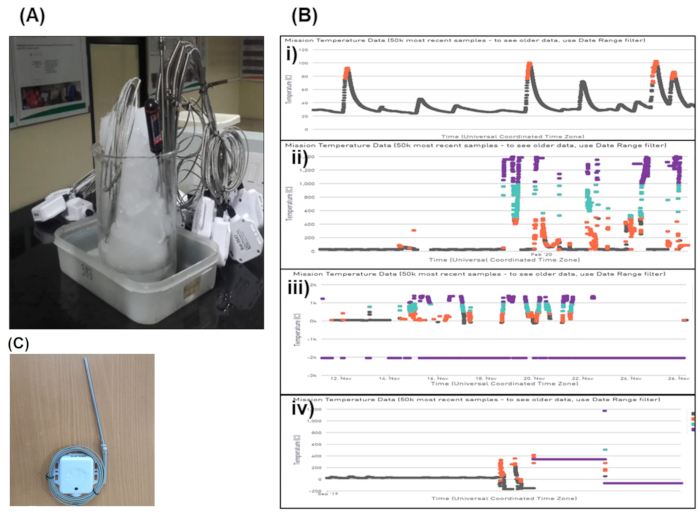
Figure 3: Stove use monitoring-temperature Loggers. (A) Calibration of Geocene Dot temperature loggers. (B) i) Valid pattern of peak for stove use monitoring; ii) Probe problem; iii) Technical error; iv) Thermocouple problem. (C) Stove use monitoring-Temperature Loggers. Please click here to view a larger version of this figure.

Figure 4: Ambient monitoring. (A) Ambient PM2.5 instrument installed at the field site. (B) Time series of ambient PM2.5 level measurements (2018-2020). Please click here to view a larger version of this figure.
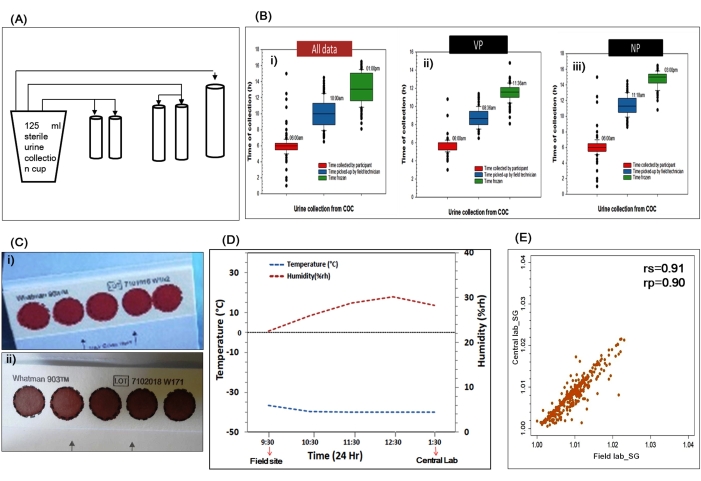
Figure 5. Biomonitoring-sample collection, processing, and quality control. (A) Urine aliquoting. (B) Chain-of-custody for sample collection, storage, and transport. (C) Dried blood spot: i) before drying; ii) after drying. (D) Cold chain-of-custody of sample shipment. (E) QA/QC of sample integrity-data of urinary specific gravity measured in the field site and central laboratory. Please click here to view a larger version of this figure.
Table 1: Valid sampling threshold criteria of PM2.5 and CO monitors. Note that due to sensitivity of the accelerometer, values outside of expected ranges were flagged but not excluded from analyses. Please click here to download this Table.
Table 2: Summary of valid DBS collection among the study participants. *During a hurricane (cyclone) there was a drop in DBS collection. †During COVID19 lockdown there was a drop in DBS collection. ‡During COVID19 lockdown there was a drop and 2021 data is not included in DBS collection. Abbreviations: M = pregnant mother; OAW = other adult woman; C = child. Please click here to download this Table.
Supplementary Table 1: Guidelines for the installation of samplers for microenvironmental monitoring.
Supplementary Table 2: Difference between the blank slot and sample slot for loading the filter. *The diffuser can be replaced only if there is any visible damage or if used for ~750-1,000 filters.
Supplementary Table 3: List of CRFs in respect to exposure and biomarker sampling. The CRFs are available in the RedCap database, stored at Emory University, and are maintained with the data-sharing agreement between all the collaborators, which can be provided to the readers upon request.
Supplementary Figure 1: Data entry sheet for filter weighing. Please click here to download this File.
Supplementary Figure 2. Instruments and steps involved in microenvironment and personal air sampling. Please click here to download this File.
Supplementary Figure 3: Cartridges and filter slots. A: Blank slot (Position 1); B: Blank bottom cartridge containing both the blank diffuser and the blank filter in the cartridge; C: Top piece of the blank cartridge; D: Sample slot (Position 2); E: Bottom sample cartridge with sample diffuser; F: Top piece of the sample cartridge. Please click here to download this File.
Supplementary Figure 4: Instruments and steps involved in stove use monitoring. Please click here to download this File.
Supplementary Figure 5: Dots installed in different cookstoves. Please click here to download this File.
Supplementary Figure 6: Instruments and steps involved in ambient air monitoring. Please click here to download this File.
Supplementary Figure 7: Instruments and steps involved in biological sampling. Please click here to download this File.
Supplementary Figure 8: Summary-of-summary of carbon monoxide (CO) data logger. Please click here to download this File.
Supplementary Figure 9: E-sampler connector layout. Please click here to download this File.
Supplementary Figure 10: Data collection and processing. Please click here to download this File.
Supplementary Figure 11: Usage of vaccine bag. Please click here to download this File.
Supplementary Figure 12: Difference between pelican and vaccine bag. Temperature performance of two cooler bags (pelican vs. vaccine) are tested using a CO data logger monitor for 48 h in the laboratory at an average room temperature of 28.3 ± 0.6 °C and RH of 49.2% ± 3.6%. A urine sample (~60 mL) with an initial temperature of 36.4 °C was placed in two bags and kept undisturbed for 48 h in a storage room. Please click here to download this File.
| BD adult lancet | BD Biosciences | 366594 | DBS collection from finger |
| BD Quikheek infant safety lancet | BD Biosciences | 368100 & 368101 | Heel prick DBS collection |
| Beacon | Roximity | O/EM | Time and location monitor [TLM] (Personal monitor) |
| Beacon Logger | Berkley Air Monitoring group | xxxx | Time and location logger [TLL] (Indirect measurement) |
Cr do ProMed Pelican Bag do ProMed Pelican Bag |
Peli Biothermal USA | Cooler bag | |
| Enhanced Children MicroPEM (ECM) | RTI International, Durham, NC, US | xxxx | Personal monitor of PM2.5 |
| E-sampler | Met One Instruments | 9800 | Indirect measurement of ambient PM2.5 |
| Geocene | Geocene Inc., Vallejo,CA | xxxx | for stove use monitoring |
| Humidity indicating card | DESSICARE, INC. | 04BV14C10 | Sample integrity indicator |
| Lascar | Lascar Electronics | EL-USB-300 | Carbon monoxide (CO) data logger |
| PTS collect capillary tubes- 40 µL | PTS collect | 2866 | To collect heel prick DBS from children |
| Sartorius | Sartorius Lab Instruments, GmbH & Co, Germany | MSA6-6S-000-DF | Microbalance (Weighing filters) |
| SootScanTM | Magee Scientific Co, Berkeley, USA | OT21 | Black carbon measurement |
| Vaccine Bag | Apex International, India | AIVC-46 | Vaccine Bag |
| Whatman 903 Protein Saver card | GE Healthcare Life Sciences | 10534612 | Collection of capillary blood samples (Dried Blood Spot) |
