Flank-propagated PDX tumors are the easiest to implant, monitor, and resect, and is generally recommended for initial establishment and propagation of PDX tumors (Figure 1). When establishing or propagating PDX tumors, it is prudent to implant tumors in multiple animals, as the tumor take rate may vary and not every piece of tumor will always take in mice. Methods have been developed for the establishment and propagation of CNS metastasis PDXs directly in the brain13. However, these methods are still more challenging with lower take rates and the tumors are significantly more difficult to propagate and monitor than flank implantation.
If patient tumors are not readily available, CNS metastasis PDX tumors can also be obtained from a variety of sources, including repositories of academic labs or commercial companies. After acquiring the tumors, the first priority would be to propagate and cryopreserve as much material as possible, ensuring a great number of low passage tumors are preserved. This ensures that sufficient material is available for an indefinite number of subsequent studies with the PDX models. Much like immortalized cell lines, PDX tumors should be cryopreserved and used at low passage numbers, as genetic drifting results in changes to the phenotype and genotype of the PDXs over time12,14,15. Regardless of the source of PDX tumors, it is important to perform frequent screening of PDX and mouse colonies for both human and mouse pathogens, such as HIV and hepatitis for humans and Corynebacterium bovis for mice. This will limit the spreading of unwanted pathogens from the PDX to both the individual handling them and other mice in the study and vivarium.
The implantation methods described here can be used to study tumor biology, evaluate multiple aspects of the metastatic cascade, and for preclinical studies. The main advantage of flank implantation is the ease of tumor monitoring over time, as tumors are visible, and its growth can be easily measured using a caliper. This method can be a good place to start for establishing feasibility of a drug target. Intracranial implantation is preferred if the presence of the brain microenvironment is important and could alter the growth or molecular profile of the tumor. In addition, intracranial implantation places the tumor behind the blood brain barrier (BBB), making it essential for preclinical studies examining the efficacy of drugs required to traverse the BBB. However, it is difficult to monitor the growth of PDX tumors and requires radiological imaging or bioluminescent imaging if the cells are labeled. Knowing when to start the drug treatment preclinically would require either imaging data to monitor growth or knowledge of average survival of mice bearing a particular PDX tumor. Furthermore, intracranial implantation bypasses all the essential steps of the metastatic cascade, making it only suitable for studying drug efficacy and tumor microenvironment within the brain. Despite the differences in the tumor microenvironment, the morphology of PDX tumors is similar regardless of the site of implantation as can be seen in this PDX tumor (CM04) derived from a brain metastasis that originated from a small cell lung cancer primary tumor (Figure 2). The small cell lung cancer morphology of tumor cells with small nuclei and scant cytoplasm can be observed in the flank tumor, intracranial tumor, and abdominal metastasis resulting from intracardiac injection. Furthermore, spontaneous metastasis from tumors implanted in the flank have been previously observed12, suggesting that the metastatic processes such as intravasation, extravasation, and colonization can be recapitulated and studied in flank tumors which would otherwise not be possible with orthotopic tumors in the brain. In general, it is observed that flank implantation is a suitable method for studying CNS metastasis biology and conducting preclinical studies.
Intracardiac injection is most often used to study organ tropism and metastatic potential of tumors. Injected tumor cells would have to undergo several steps of the metastatic cascade, including surviving circulation, extravasation, and colonization of the metastatic site. Much like orthotopic injection into the brain, it may be difficult to track the progress of tumor metastasis without radiological imaging or cell labeling. However, as with orthotopic implantation, successful inoculation results in deterioration of the condition of the animals over time as the tumor spreads. Figure 3A demonstrates metastasis to the brain after intracardiac injection in CNS metastasis PDX model, M2, which originated from a melanoma. Intracardiac injection of PDX tumor (CM04) resulted in metastasis to the abdominal cavity and liver (Figure 3B). Other organs assessed, such as the lung, kidney, and ovaries had no visible metastases.

Figure 1: Flow chart showing the general workflow of establishing, propagating, and using PDX for preclinical studies. For each inoculation method, steps of the metastatic cascade involved are listed below each method. Please click here to view a larger version of this figure.
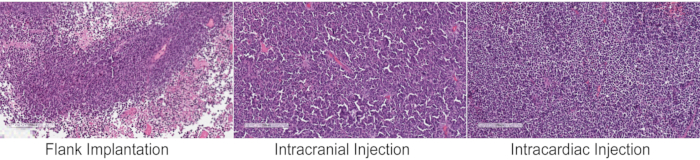
Figure 2: Histology of PDX tumors following different inoculation methods. Hematoxylin and eosin (H&E) staining of a CNS metastasis PDX tumor that originated from small cell lung cancer (CM04) implanted into immunocompromised mice by the three methods have similar tumor pathohistological and morphological features of small cell lung cancers, with small nuclei and scant cytoplasm. The intracardiac injection panel shows an abdominal metastasis. Nests of small-sized cells and high nuclear to cytoplasmic ratio is evident in all the three images. Images were taken on a slide scanner and magnified to 10x. Please click here to view a larger version of this figure.
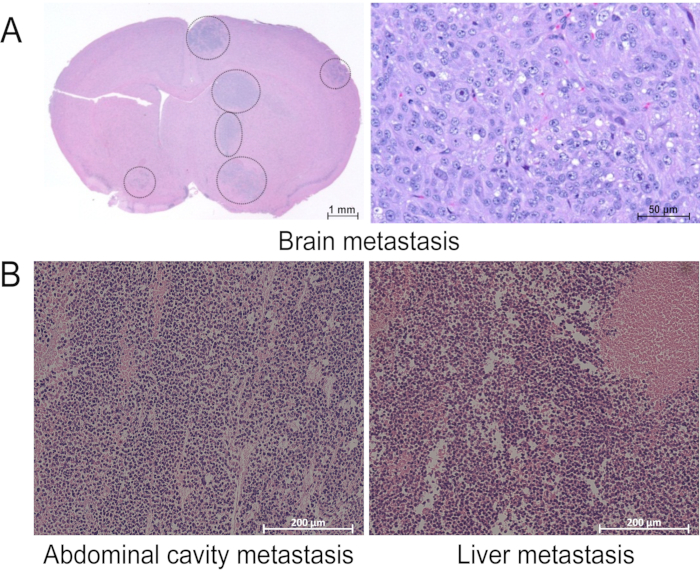
Figure 3: Metastases observed after intracardiac injection. H&E staining of tissues with visible metastasis during assessment by necropsy after intracardiac injection of (A) M2 and (B) CM04. Images were taken (A) on a slide scanner and magnified to 1x (left) or 20x (right) or (B) on a regular microscope at 10x magnification. This figure has been modified from our previous publication12. Please click here to view a larger version of this figure.
