The successful implementation of this technique relies on a few key steps to be followed. First, reliable identification of the thymus gland itself has to be ensured. In young mice, this is straightforward due to the gland's large size (Figure 3A). In older mice or immunodeficient mice, it can be more challenging; however, it is still very feasible with modern ultrasound equipment (Figure 3B,C). Second, it is critically important to set the needle trajectory so it will be visualized continuously during the advancement of the needle tip through the chest wall layers and into the thymus. A successful injection will have the needle visualized entirely while it is being advanced. This assures the operator that the needle has not traversed a critical structure, such as the heart, aorta, or one of the inferior venae cavae (Figure 4). This also applies to the injection itself. The needle tip must always be visualized in its target location during the injection so the intrathymic deposition is confirmed (Figure 5).
Some minor pitfalls exist that, if recognized, can be mitigated relatively easily. When securing the mouse to the stage and nose cone, the thorax of the mouse needs to be made as neutral as possible (i.e., without significant leftward or rightward rotation). If there is too much rotation of the thorax, the correct "approach angle" of the needle may not be easily achievable. Also, if the mouse is not secured in place tightly enough, it may move or slide when trying to advance the needle, distorting the anatomy and making visualization difficult. However, with proper technique and preparation, a successful intrathymic injection can be achieved with consistency, reliability, and reproducibility.
Once the injection is complete, there are multiple ways to confirm the intrathymic location of the injection. The present study used luciferin as an injectate into luciferase transgenic mice. These can then be evaluated immediately following the injection with bioluminescence imaging, confirming the injection's correct location without sacrificing the animal (Figure 6A). This technique has the additional advantage that injected luciferin-tagged cells can be imaged at multiple time points, ensuring the persistence of activity in the thymus. Alternatively, trypan blue can be injected as a visual marker of the injection site, and injection accuracy can then be confirmed ex vivo with necropsy16 (Figure 6B).

Figure 1: Anesthetized mouse positioned on the imaging stage for ultrasonography of the thymus. A 6-week-old female C57BL/6 mouse with a depilated chest was anesthetized and transferred to the imaging station. The mouse is in a supine position, with the outstretched legs secured by tape. Please click here to view a larger version of this figure.

Figure 2: Ultrasound machine settings. Image of the ultrasound machine control panel (touch screen). The main adjustments of the settings to optimize imaging will be adjusting the depth (red arrow), the focal zone (circled in yellow), and the gains (red asterisk). Please click here to view a larger version of this figure.
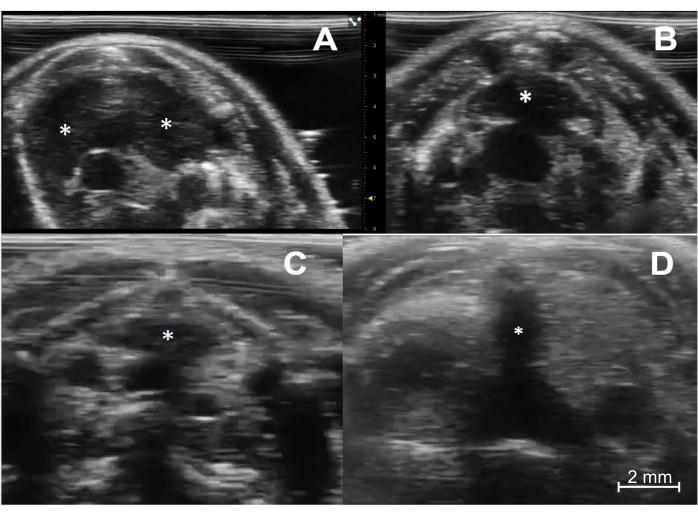
Figure 3: Ultrasound imaging of the thymus in immunocompetent and immunodeficient young and aged mice. (A) Immunocompetent young mouse (C57BL/6, female, 4 weeks old, n = 5). The transverse sonographic view shows the thymus's right and left lobes (asterisks). (B) Immunocompetent aged mouse (C57BL/6, female, 6 months old, n = 5). The thymus (asterisk) is smaller but maintains its typical location and pyramidal shape. (C) Immunodeficient young mouse (NOD scid gamma, female, 4 weeks old, n = 5). Note the much smaller size of the thymus (asterisk) compared to the normal young mouse. (D) Athymic nude mouse (female, 8 weeks old, n = 1). There is a complete absence of thymic tissue. Of note, the dark (hypoechoic) vertical line in the middle of the image (asterisk) is a shadowing artifact from the sternum, with no true thymic tissue. Please click here to view a larger version of this figure.
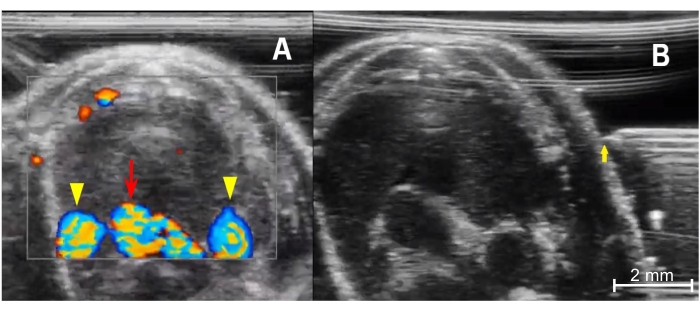
Figure 4: Preparing for injection. (A) Color Doppler image of the anterior thorax demonstrates the thymus's relationship with the mediastinal vessels. The bottom center is the aortic arch (red arrow), and the rounded vessels on either side are the right and left superior venae cavae (yellow arrowheads). Blood flowing toward the imaging probe is encoded in red, and blood flowing away from the transducer is encoded in blue. (B) Needle placement from prior to advancement into the chest from a left-sided approach. The needle tip (yellow arrow) must be in line with the ultrasound transducer and the tip level with the mid portion of the thymus. Please click here to view a larger version of this figure.
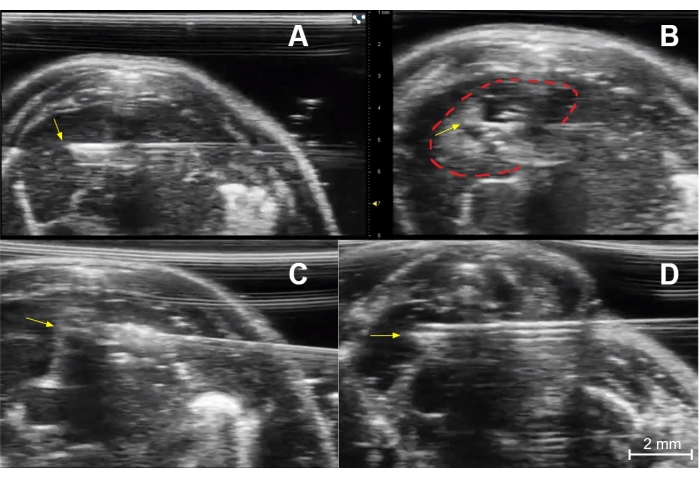
Figure 5: Injection technique. (A) Needle placement for injection of the right thymic lobe of an immunocompetent young mouse. The needle tip (yellow arrow) is in the central portion of the right lobe. (B) Post-injection image of the right lobe showing a collection of dark (hypoechoic) fluid and small bright (echogenic) air bubbles at the injection site (dashed red line). The yellow arrow indicates the needle tip. (C) Needle placement (yellow arrow at needle tip) for injection of the left thymic lobe of an immunocompetent young mouse. (D) Needle placement (yellow arrow) for injection of the right lobe of an immunocompetent young mouse. Please click here to view a larger version of this figure.
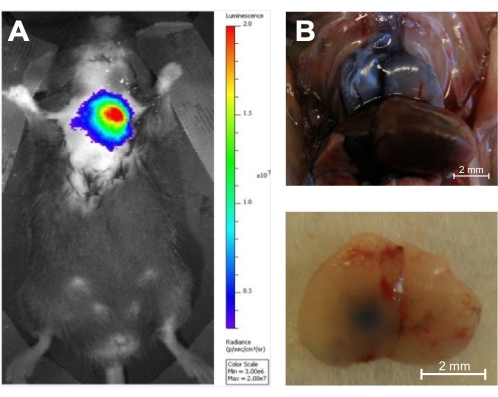
Figure 6: In vivo and ex vivo verification of accuracy. (A) Injection of D-luciferin (0.1 μg/10 μL) into the thymus of an 8-week-old luciferase transgenic mouse followed by 1 s of in vivo bioluminescence imaging using an in vivo bioluminescence imaging system (n = 3). The color coding shows the total bioluminescence radiance (photons·s−1·cm−2·steradian−1) as indicated by the color bar on the right. (B) The thymus of two 5-week-old C57BL/6 mice was injected with trypan blue, and the injection accuracy was demonstrated by necropsy (n = 3). Top panel: Dorsal surface of a Trypan Blue-stained injected thymus in situ. Bottom panel: Ventral surface of a Trypan Blue-stained thymus ex situ after injection of the left lobe. Reproduced with permission from Tuckett et al.1. Please click here to view a larger version of this figure.
