This protocol will allow an investigator to determine confidently whether a mouse is pregnant, including during the early stages and to determine whether there are obvious prenatal embryonic or fetal losses without needing to sacrifice the pregnant dam. This protocol is especially useful when breeding genetically engineered mice; typically, heterozygous x heterozygous crosses to yield homozygous offspring leads to failure of proper development, which causes prenatal lethality. Figure 1 depicts a representative situation in which embryos progressively die and then are resorbed through mid-gestation. Figure 2 shows how to find the left and right uterine horns by following the vagina up through its bifurcation. Figure 3, Figure 4, Figure 5, Figure 6, Figure 7, Figure 8, and Video 3 show mouse embryos at various stages of development. Early-stage mouse embryos, dead embryos, or resorbed embryos may resemble other organs in the abdomen or feces in the intestines, or conversely, intestinal loops may mimic the non-gravid uterus. Figure 9 and Figure 10, as well as Video 4 and Video 5, demonstrate such potential imaging artifacts that may mimic the gravid uterus, for which the investigator must be on alert.
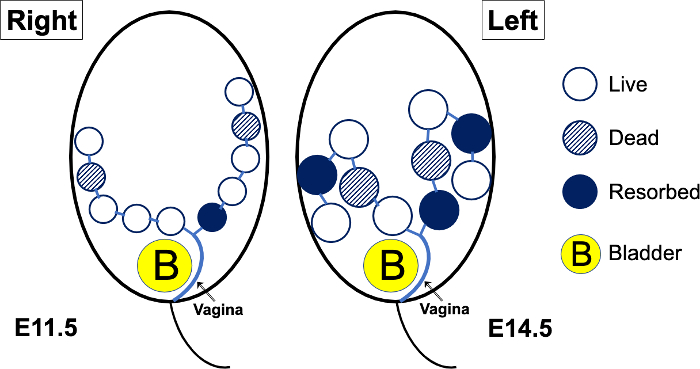
Figure 1: Schematic diagram of a theoretical pregnant mouse abdomen, imaged at E11.5, then again at E14.5. Up to mid-gestation (E10.5 or E11.5), the mouse embryos will be positioned along the right and left peripheral aspects of the abdomen. As the embryos grow, the more distal portions of the uterus and their corresponding embryos will turn outwards and posteriorly. As the embryos grow further (E15.5 and later, generally), the mouse fetuses will be positioned almost randomly in various directions, and it becomes difficult to “track” a uterus from proximal to distal. When there is prenatal lethality in a genetically engineered mouse model, the embryos (open circles) may die; the dead embryos (hatched circles) will eventually become resorbed (solid circles). Please click here to view a larger version of this figure.
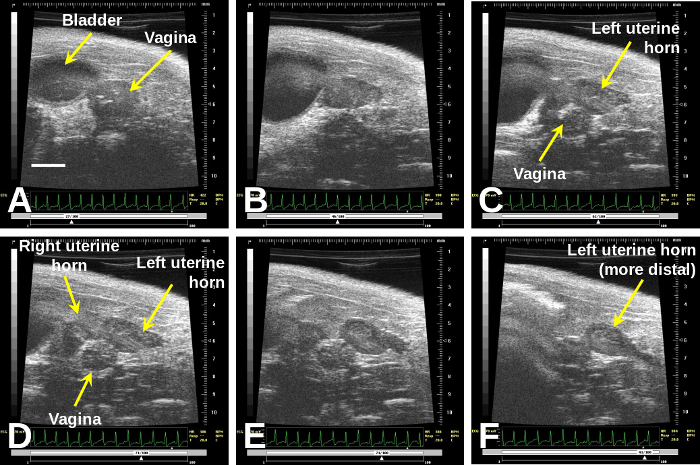
Figure 2: Once one finds the vagina (A), immediately to the right of the bladder, sweeping cranially will demonstrate the bifurcation (B) to the right and left uterine horns (D)–(F).
Scale bar (A) = 2 mm. Please click here to view a larger version of this figure.
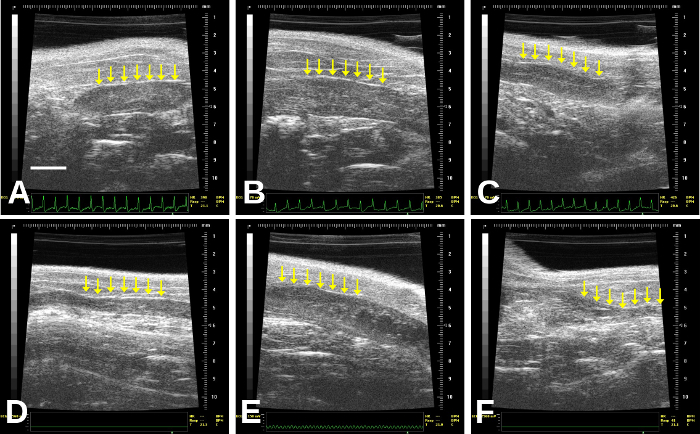
Figure 3: Images of non-gravid (non-pregnant) uterus (identified by the rows of arrows). The uterus may vary in thickness: thicker in (A), (B), (E); thin with a central thin echogenic line (C), very thin (D), or may even contain small, cystic structures that should not be mistaken for concepti (B) and (E) especially, although this may be difficult to determine. (A) is a right uterine horn; this is more difficult to follow distally in our experience due to bowel gas. (B)–(F) are left uterine horns; (F) is quite distal/lateral and so becomes more difficult to image due to increasing bowel gas artifact. Scale bar (A) = 2 mm. Please click here to view a larger version of this figure.
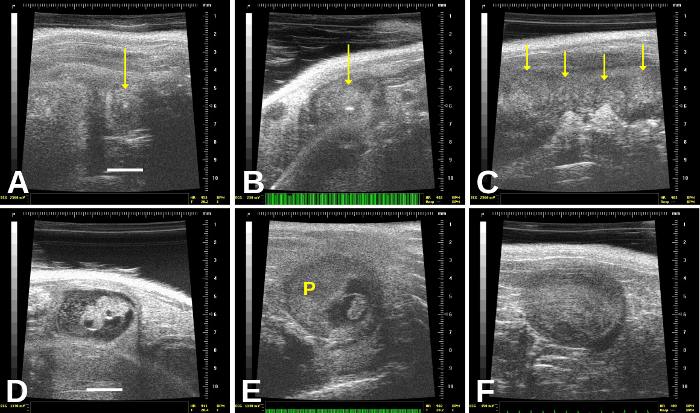
Figure 4: Resorbed and dead embryos have distinct appearances. Resorbed embryos, which are very commonly found, are encased within a round (gravid) uterine sac that appears relatively homogeneous except for a central echogenic (very bright) “spot”—arrows in (A) and (B). (C) shows resorbed or dead embryos; there is an entirely homogeneous, “mushy” appearance to the uterus, and we see probably 3–4 dead embryos in this frame. (D) shows a recently dead embryo, which still shows some structures; there also appears to be cellular debris in the amniotic sac. In (E), the dead embryo is much shrunken and still connected to the placenta (“P”). (F) shows a homogeneous, “mushy” appearance of an embryo that probably died 1–2 days previously, but is not yet completely resorbed. Scale bar for (A) and (D) = 2 mm. Please click here to view a larger version of this figure.
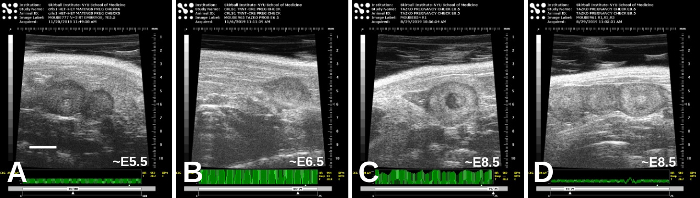
Figure 5: Early-stage embryos, from approximately E5.5 (A) and E6.5 (B) to E8.5 ((C) and (D)). There are variations in appearances, and the estimated stages here were based on timing of mating as well as the appearance of the embryos themselves. Scale bar (A) = 2 mm. Please click here to view a larger version of this figure.
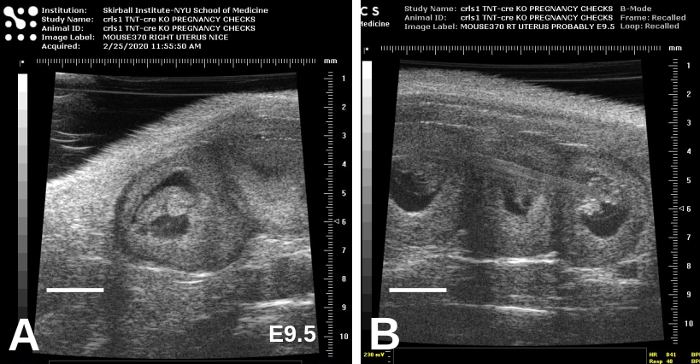
Figure 6: E9.5 embryos are considerably larger than E8.5 embryos and are beginning to take form. Representative images, showing adjacent embryos, are shown in (A) and (B). Scale bars = 2 mm. Please click here to view a larger version of this figure.
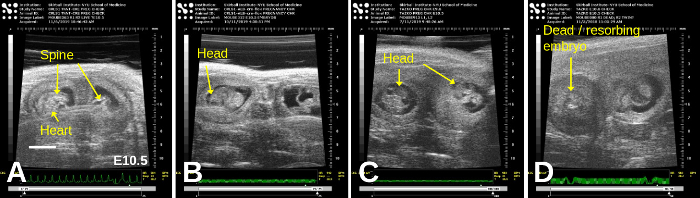
Figure 7: E10.5 embryos exhibit even clearer organs such as the head, spine, and heart. Representative images, showing adjacent embryos, are shown in all panels; in (D), a dead/resorbing embryo lies adjacent to a live embryo. Scale bar = 2 mm. Please click here to view a larger version of this figure.
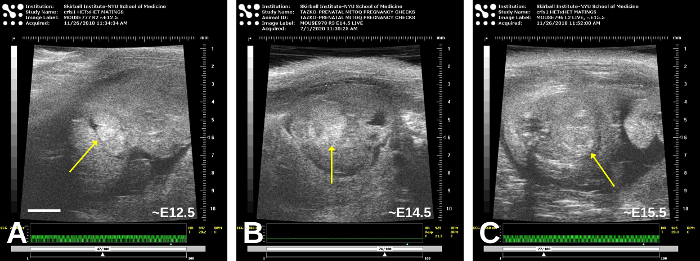
Figure 8: Older embryos, approximately E12.5 (A), E14.5 (B), and E15.5 (C). Oblique planes of imaging obscure the precise anatomy somewhat, but the heart (arrow) is in the central portion of each embryo; in (C), the myocardium is now more echogenic than the blood. Please click here to view a larger version of this figure.
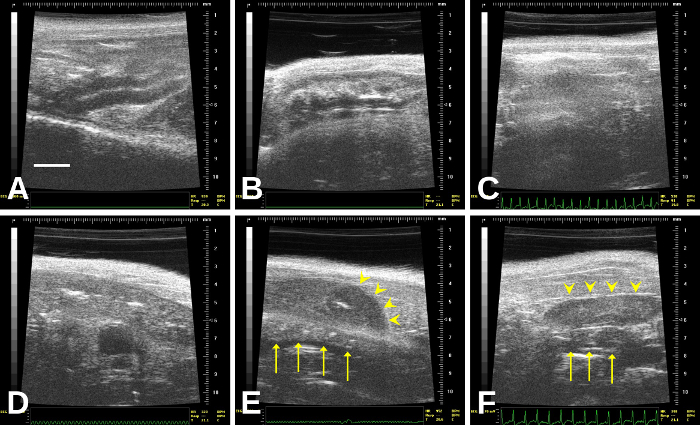
Figure 9: The bowel, which is the organ most likely to be confused with the uterus. In (E), a resorbed embryo (arrowheads) overlies a segment of bowel (arrows). In (F), a non-gravid uterus (arrowheads) overlies a short segment of bowel (arrows) Please click here to view a larger version of this figure.
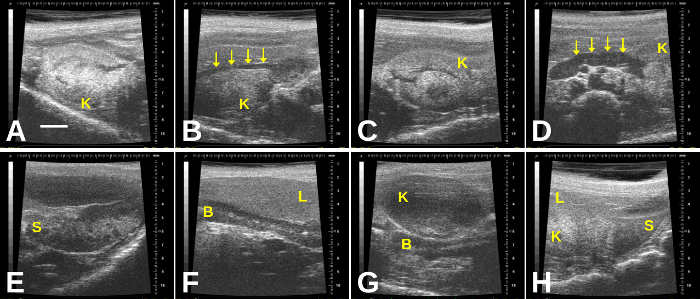
Figure 10: Additional imaging artifacts in the gravid abdomen include the kidneys, spleen, and liver. (A) Right kidney; (B) Right kidney with renal artery (arrows); (C) Left kidney; (D) Left kidney with renal artery (arrows); (E) Spleen; (F) Liver overlying a segment of bowel; (G) Kidney overlying segment of bowel; (H) Spleen, liver, and left kidney seen in one plane of imaging. B = bowel; K= kidney; L= liver; S= spleen. Scale bar (A) = 2 mm. Please click here to view a larger version of this figure.
