We have adapted this protocol for use in MS. We targeted the delivery of ten tDCS stimulation sessions delivered over two weeks. 9,10 The first two sessions of the ten were in-person training sessions and the following eight were remotely supervised (Figure 3). The second session consists of an environmental suitability assessment where study technicians visited the participant's home to confirm appropriate set-up.
To complete the following remotely-supervised sessions, participants were provided with the tDCS device specially-designed for remote use and a headset that was modified for ease of use to guide accurate electrode placement. A device kit was provided and included the device and headset, one-time use sponge pockets for electrodes and syringes filled with the measured amount of saline required for each sponge, with all items individually labeled by day and organized for ease of use. Electrodes were placed in the bilateral dorsolateral prefrontal cortex (DLPC) position with the anodal electrode placed on the left side. 10 This offers ease of reliable electrode placement, wide therapeutic applications.9,10 Based on prior studies we targeted 1.5 mA for 20 min sessions. The protocol 9,10allowed for a current reduction to 1.0 mA at baseline if this improves overall subject tolerability.
Participants were given a study-provided laptop computer configured for the study, including the easily accessible instructional video and link for secure video conference connection with the study technician. The laptop also included a program for remote monitoring of all computer activity, and a program to remotely access the computer for technical support. Detailed manuals for operation were used by both the participant and study technician, and a binder for self-report measures was provided.
A total of n=20 MS participants have completed the study. Inclusion criteria specified an Expanded Disability Status Scale (EDSS)25 * of 6.0 or below OR 6.5 or above with proxy to ensure minimal motor requirements to operate the device. Enrollment has been representative of a range of impairment in MS (motor impairment, cognitive impairment, or both). All 20 participants, n=4 with proxy, were successfully trained to self-apply a tDCS session and 192 total sessions were completed. As shown in Figure 4, 40 of the192 sessions included training; the remaining 152 were exclusively remotely-supervised sessions. Of the remotely-supervised sessions, 100% were executed correctly with successfully placement of electrodes, device operation and well-tolerated delivery of stimulation.
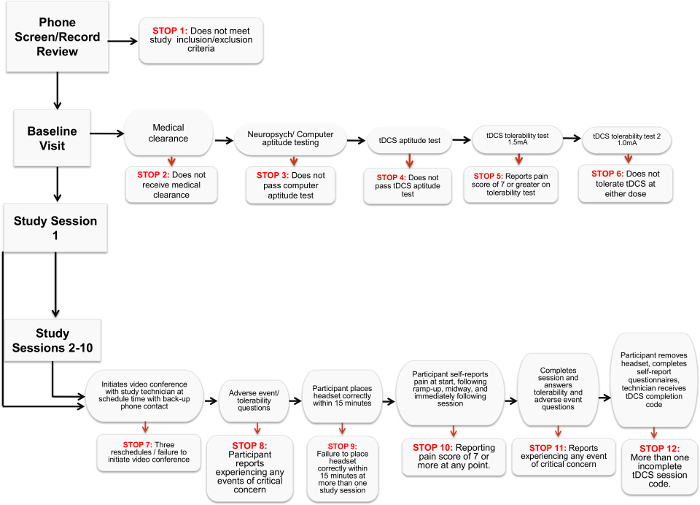
Figure 1. Stop Criteria Flowchart. The chart details the various criteria that indicate a participant can no longer proceed or participate in a remotely-supervised tDCS study. Please click here to view a larger version of this figure.
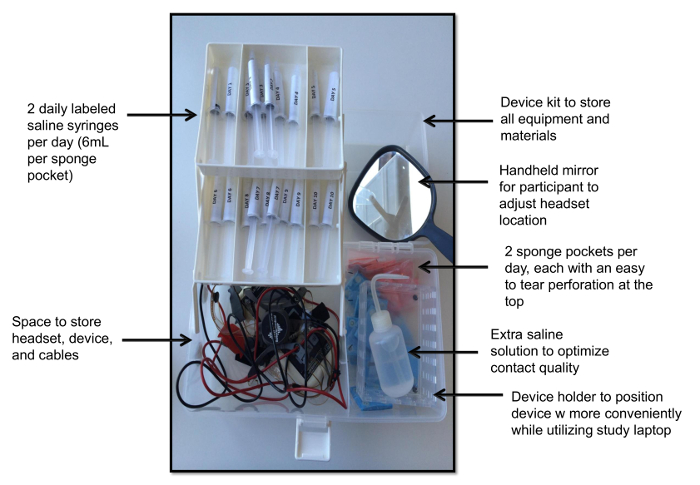
Figure 2. Device Kit. This view demonstrates the device kit with individually wrapped sponge pockets, one saline-filled syringe per sponge per day, a handheld mirror a device holder, spare saline solution, and the device with headgear. Please click here to view a larger version of this figure.
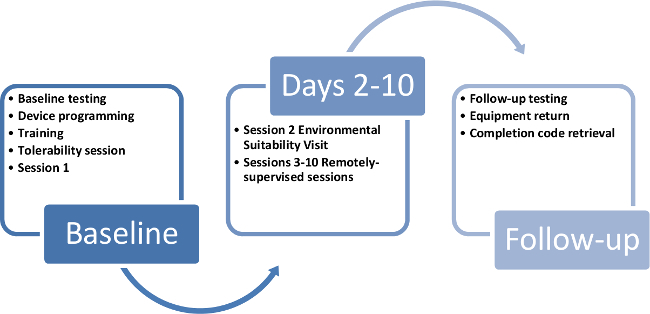
Figure 3. Participant study timeline. This timeline demonstrates a way to cycle study kits and devices through each 10 day participant enrollment in the study. Please click here to view a larger version of this figure.
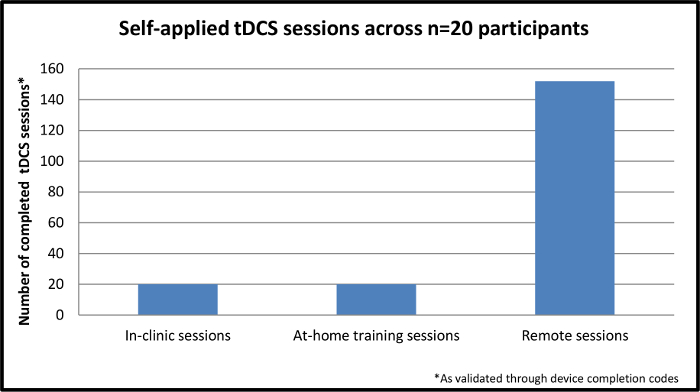
Figure 4. Self-applied tDCS sessions across n=20 participants. This figure demonstrates the completed, self-applied sessions across n=20 participants enrolled in the study. The initial session is completed in-clinic while the remaining nine sessions are completed through remote supervision in the participant's home. Please click here to view a larger version of this figure.
