The DBS procedure and invasive recordings were approved by the Ethics Commission of the University Clinic Düsseldorf, Germany.
1. Experimental Paradigm Design and Patient's Consent
NOTE: Design an experimental paradigm or select an existing experimental paradigm to target a cognitive/emotional aspect of interest.
- Select patients that will undergo DBS-treatment. Ask if the DBS-Patient meets the study's inclusion criteria. If yes, obtain signed informed consent from patient and/or ethical commission (if applicable) to carry out a post-operative recording and application of the respective cognitive paradigm.
Note: Post-operative recording takes place the following day after an initial DBS surgery is carried out for DBS electrode implantation (together with their corresponding externalization from the head by means of special cables) and before a second surgery takes place regarding permanent implantation of DBS electrodes and stimulator.- In the Flanker task (Example 1), obtain signed informed consent from a patient with movement disorder (e.g. Huntington's or Parkinson's disease) in order to carry out a post-operative recording. The goal of the Flanker experiment is to test the patient's ability for adaptation to error behavior and to determine how such adaptation is reflected on brain oscillatory activity at the cortical and subcortical level.
NOTE: The choice of a patient is dictated by the cognitive mechanism to be addressed and the patient's disorder. In the DBS-DOC case-example (Example 2), a female DOC patient who suffered from a head injury at the age of 38 was selected. Because of the patient' condition limiting informed consent, DBS treatment and experimental participation was approved solely by the local ethics commission. The main goal of the DOC postoperative recording was to determine whether brain function in relation to cognitive-emotional processing was still intact in a patient with such severe disorder of consciousness.
- In the Flanker task (Example 1), obtain signed informed consent from a patient with movement disorder (e.g. Huntington's or Parkinson's disease) in order to carry out a post-operative recording. The goal of the Flanker experiment is to test the patient's ability for adaptation to error behavior and to determine how such adaptation is reflected on brain oscillatory activity at the cortical and subcortical level.
- Choose between the type of stimulus to be presented (auditory, visual). Identify the order of stimulus presentation (block or mixed design). Select the duration of stimulus, inter stimulus interval (ISI) and the number of trials.
- As one practical example perform the Flanker task (Example 1, Figure 1A), to examine the ability to adapt behavior in response to the commitment of response errors. This task consists of visual stimuli (flanked arrowheads vertically arranged).
- Flank the target stimulus (arrowhead in the center) by two adjacent arrows (above and below target) either pointing in the same (compatible) or opposite (incompatible) direction, additionally consider stop trials (circle in the center).
- Present the target to the left or right, and ask the participant to press a response button with their left or right thumb. In the stop trials, instruct the participants not to respond. Present flankers 200 msec before target. Display the target for 300 msec and set the response stimulus-interval to 2,000 msec (elapsed time is indicated by a cue tone). Present a total of four blocks of 120 stimuli each in this task. Present compatible (60%), incompatible (20%) and stop-trial (20%) stimuli randomly.
NOTE: This value for the stimulus-interval was chosen to avoid a large number of missed trials when considering motor disabled patients. Flankers and target were switched off simultaneously. Patients were instructed to respond as quickly as possible.
NOTE: In the DBS-DOC case-example (Example 2, Figure 1B), the experimental paradigm consisted of neutral non-addressing and familiar-addressing speech stimuli26 in a block design. The stimulus duration was set-up to 4 sec (with a randomized 4 5 sec inter-stimulus-interval). A total of 80 trials per condition were considered in this paradigm (Figure 1B).
- Envision the patient's physical constraints and needs in a post-operative setting recording. Specifically, determine if the patient is able to make use of the computer keyboard by considering the presence of excessive chorea movements (Huntington's disease) or tremor (Parkinson's disease).
- Make sure the patient is able to see the monitor (as the local anesthetic or the stereotactic head frame applied during DBS surgery may have caused swelling in the face and around the eyes) and sit comfortably during the duration of the whole experiment. Do not perform the experiment, if the patient fails to meet these conditions.
2. Set-up for Postoperative Subcortical (LFPs) and Surface (EEG) Recordings
- Set up the EEG equipment (see Materials in the supplementary files) in the room where the experiment will be conducted. Connect the recording computer to the EEG system. Start the EEG recording software (see "materials" in the supplementary files).
- Click "File" and then "New workspace" to define the workspace in the EEG recording software by specifying: a sampling frequency of 5 kHz, a low cut-off (DC) and high cut-off frequency (1,000 Hz), EEG channels according to the international 10/20 system (at least: fronto-central (Fz), centro-central (Cz), fronto-polar reference (Fpz) and ground (mastoid) and depending on the paradigm furthermore parieto-central (Pz), occipito-central (Oz), temporal (T3/T4), fronto-medial (F3/F4), fronto-lateral (F7/F8) ) (Figure 2D) and LFP channels (LFPL 0, LFPL1, LFPL2, LFPL3 (left hemisphere, Figure 2C); LFPR0, LFPR1, LFPR2 and LFPR3 (right hemisphere)). Click "Monitor" to verify that the specified channels are now set up for recording.
NOTE: The preparation beforehand of the workspace is recommended in order to minimize the experiment time and to oversee unexpected changes in the recording's configuration. It is recommended to ensure the highest temporal resolution, correct filter settings, adequate sampling rate and proper selection of channels of interest. - Set up the stimulus computer by connecting the parallel port to the EEG system. Start the stimulus software. Click "run" to check the paradigm's functionality on the computer's monitor (visual stimuli) and/or speakers (auditory stimuli, sound cues). Make sure markers (triggers) from the stimulus computer are read into the recording system during presentation of stimuli and subject's response by checking their appearance on the EEG recording software.
NOTE: Triggers from stimulus devices must have duration of at least 200 µsec to be detected by the EEG system (with the 5 kHz sampling rate). Since triggers are markers of event-related-events or evoked related activity that occur at a specified period of time their function is crucial for posterior data analysis. In the DBS-DOC case-example (Example 2), the experimental paradigm (Figure 1B) consisted of auditory stimuli (familiar an unfamiliar voices) so triggers were set up at the beginning and end of each stimuli presented. In the case of the Flanker task (Figure 1A) triggers were set up at the instant when 1) the flankers and target stimuli appeared, 2) the patient responded and 3) a cue tone was heard to inform the patient that the response-time had elapsed. - Mark the vertex of the patient's head as the midpoint between the nasion and inion by using a skin marker pen and by following the advice of an experienced neurologist or EEG specialist. Additionally, mark chosen EEG electrode positions using the 10-20 system. Attach EEG surface electrodes to the scalp by first cleaning each selected location with an isopropyl alcohol pad and after the use of abrasive paste.
NOTE: Such actions are constrained by the placement of bandages on the head of the DBS patient. However, an experienced neurologist should be able to define an appropriate (approximate) location for each electrode/channel. To ensure proper contact move hair out of the way (if applicable). The use of self-adhesive electrodes secured by surgical tape might be used due to easiness of placement. - Connect externalized DBS electrodes to a percutaneous extension. Connect percutaneous extension to external cable connector. Connect each electrode provided by the external cable connector to the EEG control box according to the EEG recording set-up. Connect EEG scalp electrodes to the EEG control box by first plugging ground and reference.
- Attach EMG electrodes (reference and active electrodes) at specified muscles by first cleaning the area with an isopropyl alcohol pad. Connect EMG electrodes to EEG control box.
NOTE: This step is optional and mainly conducted when motor tasks are considered into the paradigm or when it is required to monitor the activity of muscles as in the case of patients with motor disorder. - Click "Monitor" to visualize data. Make sure EEG and EMG signals displayed on the monitor are artifact-free by detecting the presence of jittering and superimposed high frequency components. Check guidelines about types of artifacts and other factors related to recording electroencephalographic signals35 and/or request technical advice from an experienced neurologist or neuroscientist until you become familiar with the type of disturbances present in such physiological recordings.
NOTE: This step is important to ensure high quality signals for off-line data analysis.
3. Recording of Post-operative Subcortical (LFPs) and Surface (EEG) Brain Activity
- Provide instructions to the patient. Make sure the patient is comfortable and instruct him/her to stop the experiment at any time of discomfort.
- Click "run" on the stimulus software so that the patient is able to see the paradigm on the monitor and/or listen to the cue tones and sounds. Perform a training session with the patient until he/she is comfortable with the task. Start simultaneous recording of subcortical (LFP) and cortical (EEG) brain activity while the patient performs the experimental task.
NOTE: In the case of the DBS-DOC case example (Example 2) the paradigm consisted of auditory stimuli in a block design as described in (Figure 1B). In the case of the Flanker task (Figure 1A), visual stimuli corresponding to three conditions (compatible (60%), incompatible (20%) and stop-trial (20%)) were presented randomly within each block (mixed design), each block consisted of 120 stimuli and the paradigm consisted of a total of four blocks. After the task has been finalized, data is stored on the hard disk of the recording computer for later off-line screening and quantitative analysis.
4. Data Analysis
NOTE: Steps by using EEG analysis software:
- Open the EEG analysis software (see "materials" in the supplementary files) and click "New" to visualize the recorded data by specifying the folder paths (raw, history and export) and data's name. Click "Edit channels" to select channels of interest. Rename channels if necessary.
- Click "Channel Preprocessing" and then "New Reference" to re-reference adjacent DBS contacts and thus create virtual bipolar contacts for left and right hemispheres. Repeat this process to create a virtual montage for EEG channels.
NOTE: A bipolar re-reference montage is important to minimize volume conduction effects and to improve spatial reliability of the recorded signals. In the case of the DBS-DOC case example (Example 2), the following bipolar channels were set-up DBS: LFPL01, LFPL12, LFPL23, LFPR01, LFPR12, LFPR23 and EEG: Cz/Fz, Pz/Cz, Oz/Pz, T3/Cz and T4/Cz. It is worthy to emphasize that while MEG recorded signals are reference-free, EEG signals need to be referenced to set true non-arbitrary zero value signals in a common framework. Existing EEG reference systems include: Cz or FPz reference, average between electrodes on the two ears, average reference (considering all of the channels), two- or single-mastoid reference and noise reference. For the purpose of data analysis, different re-reference arrangements can be utilized, for instance bipolar contacts are appropriate when targeting time-frequency coupling analysis between DBS and EEG signals. - Click "raw data inspection" to screen data for physiological and equipment related artifacts with emphasis on motor jittering and equipment disturbances. Mark segments in which artifacts are present.
NOTE: When recording scalp activity and simultaneously subcortical activity through DBS externalized leads, EEG appears more robust to noise artifacts than techniques such as MEG for which current efforts are being directed towards improving signal to noise ratio. Due that patients with motor disorders suffer from involuntary movements such as chorea and tremor the appearance of motor jittering artifacts in the recorded signals needs to be accounted for. Other disturbances are due to eye blinks and equipment related artifacts. Focusing on the DBS-DOC case example (Example 2), artifact inspection was performed by visual examination and artifacts were manually marked. The sole application of an automatic artifact inspection mode is discouraged as some artifacts may not be recognized by a specified criterion. - Click "Data Filtering" and then "IIR Filters" to specify a notch filter: 50Hz (dealing with power line artifacts) and Butterworth Zero Phase Filters by specifying Low and High Cutoff parameters. Click "Change Sampling Rate" to downsample the recorded signals to a specified frequency and also specify the interpolation type.
- In the DBS-DOC example; set Low Cutoff: 1.0000 Hz, Time constant: 0.1592s, slope: 48 dB/oct; High Cutoff: 80.0000 Hz, Time constant: 0.1592 sec and 48 dB/oct and downsampling frequency to 512 Hz by using spline interpolation.
NOTE: Optionally, perform filtering by customized scripts based on well-known open source suites: Fieltrip (http://www.fieldtriptoolbox.org/), EEGLab (http://sccn.ucsd.edu/eeglab/) and SPM8 (http://www.fil.ion.ucl.ac.uk/spm/software/spm8/). In the case of the first, sample scripts are provided in (http://www.fieldtriptoolbox.org/tutorial/preprocessing). Other suites also provide detailed documentation to carry out this step.
NOTE: Down-sampling at any point will limit the frequency space that is available for further analysis according to the Nyquist theorem. Considering the DBS-DOC case-example, the selected sampling frequency of 512 Hz is appropriate when considering a frequency band up to 80 Hz.
NOTE: Alternatively, perform down-sampling by customized scripts based on well-known open source suites: Fieldtrip (http://www.fieldtripbox.org), EEGLab (http://sccn.ucsd.edu/eeglab) and SPM8 (http://www.fil.ion.ucl.ac.uk/spm/software/spm8/). In the case of the first, script examples are provided (http://www.fieldtriptoolbox.org/tutorial/preprocessing). Other suites also provide documentation to carry out this step.
- In the DBS-DOC example; set Low Cutoff: 1.0000 Hz, Time constant: 0.1592s, slope: 48 dB/oct; High Cutoff: 80.0000 Hz, Time constant: 0.1592 sec and 48 dB/oct and downsampling frequency to 512 Hz by using spline interpolation.
- Export bipolar channels of interest by clicking "Export" and then "Generic Data". Export data markers (triggers) by clicking "Export" and then "Markers". Name the files to be exported by selecting a "txt" format.
NOTE: In order to use the Fieldtrip toolbox in the next steps it is suggested to export channels in (.txt) multiplexed format and also recommended to include a "vmrk" file that includes info about exported channels. It is also suggested to use a (.txt) format for the exported markers while the option of skipping markers corresponding to bad intervals selected in step 4) is offered.
NOTE: Steps by using Fieldtrip:
- Start-up MATLAB and click on "set path" to add the Fieldtrip folder's path in case it is not done by default.
- Put the data previously pre-processed and markers into a cell-array-structure that is compatible with the functions within Fieldtrip by running (Script 1-Supplementary File) without missing to specify: The directory that contains the EEG and LFP files from step 7, channel names, sampling frequency, sample time, trials. (Optionally) Perform artifact rejection by "uncomment" the indicated code. This script saves the data into a specified file that will be used in the next steps.
- Calculate LFP's spectral power for channels of interest by running (Script 2-Supplementary File) without missing to specify: the directory that contains the file generated by (Script 1), the method (wavelet or mtmconvol), the width of the window, the frequency of interest (foi), time's period of interest (toi), and frequency baseline correction (optional). Define the type of statistical analysis and desired p-value.
Note: In the DBS-DOC case-example (Example 2), power analysis was performed by considering a stimulus-locked wavelet time frequency analysis (Morlet wavelet (width = 5)) with Hanning taper, a frequency range of 4-80 Hz and a time period between -1 to 4 sec. Due that wavelets have variable resolution in time and frequency. When selecting a wavelet, we decide a trade-off between temporal and spectral resolution. In particular, Morlet wavelets possess a sinusoidal shape weighted by a Gaussian kernel that enables capturing local oscillatory components in a time series. Making the width parameter smaller will increase the temporal resolution at the expense of frequency resolution and vice versa. The spectral bandwidth at a given frequency F is equal to F/width x 2 (for F = 40 Hz and width = 5 the spectral bandwidth is 16 Hz) while the wavelet duration is equal to width/F/pi (for F=40 Hz and width=5 the wavelet duration is 39.8 msec). A cluster based (time and frequency variables) randomization approach was used for statistical analysis between conditions (p-level of .05 in a two-sided test) 39. As an example of the output obtained by performing this step please look at Figure 4A and Figure 4D. Time-frequency response analysis was performed by customized scripts based on the open source software Fieldtrip (http://www.fieldtriptoolbox.org/). Specific details about how to customize a script to accomplish this step can be found in http://www.fieldtriptoolbox.org/reference/ft_freqanalysis. - Calculate coherence between subcortical and cortical signals by running (Script 3-Supplementary File) without forgetting to specify: segments length, overlap percentage, frequency of interest. As for the statistical analysis specify the type of analysis and desired p-value.
Note: Coherence analysis measures the linear relationship between two time series with a constant ratio of amplitudes40. In the DBS-DOC case-example (Example 2), segments of 1 sec with 50% overlap were used for the calculation of coherence by focusing on the frequency interval between 1 and 25 Hz. A cluster-based (time and frequency variables) randomization approach was used for within-subject analysis of coherence (p-level of .05 in a two-sided test)41. Furthermore, the imaginary part of coherence was computed42.
The basic steps to customize a script for coherence analysis are described in (http://www.fieldtriptoolbox.org/tutorial/coherence). As an example of the output obtained by performing this step please look at Figure 4B. - Calculate cross frequency phase amplitude coupling (PAC) by running the software implementation available as supplementary file in reference43.
Note: In the DBS-DOC case example (Example 2), cross-frequency analysis PAC was calculated by using the entire free-artifact recording for different combinations of bipolar channels. In particular, normalized direct PAC (ndPAC)43 was preferred because it enabled determination of significant coupling at different statistical levels while setting-up to zero the non-significant couplings (p-level: 0.1). As a result, frequency ranges for phase and amplitude coupling could be selected on the basis of their significance. In the DBS-DOC case example, the phase frequency range considered was 3-22 Hz while the amplitude frequency range was set up to 35-80 Hz. The LFP-EEG channels selected for PAC analysis were LFPR23 and EEGFzPz on the basis of the coherence analysis performed in step 5.5. As an example of the output obtained by performing this step please look at Figure 4C.
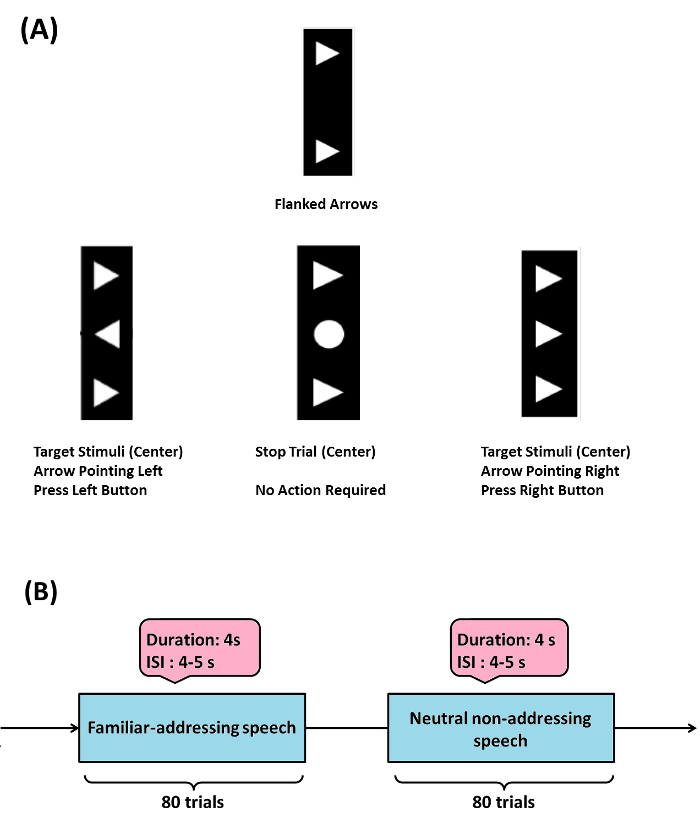
Figure 1: Sample Experimental Paradigms. (A) (Example 1) Flanker task: target stimulus (arrowhead in the center) is flanked by two adjacent arrows (above and below target) either pointing in the same (compatible) or opposite (incompatible) direction, stop trials (circle in the center) were also considered. When target is pointed to the left or right, a participant has to press a response button with their left or right thumb respectively, in the stop trials participants are instructed not to respond. The Flanker task used here was modified from the initially programmed version by Prof. C. Beste and his group (please see acknowledgements). (B) (Example 2) emotional-cognitive speech paradigm used in the DBS-DOC case-example. Please click here to view a larger version of this figure.
For the DBS-DOC case (Example 2), we now provide data on target localization for DBS implantation, schematic diagrams of LFP electrode and EEG set up, exemplary recordings of EEG and LFP activity (raw data) and representative analysis results:
Figure 2A shows planned trajectory (black line) projected on an anatomic atlas36, section 30, coronary, 10.7 mm behind the anterior commissure (AC) (red line: AC-PC plane). Red circles mark targeted areas of the lowermost 15 mm (atlas grid size: 10 mm) with iml = internal medullary lamina thalami and Rt = reticular thalamic nucleus. VA = ventroanterior thalamic nucleus, AV = anteroventral thalamic nucleus, AM = anteromedial thalamic nucleus, Fa = fasciculosus nucleus, IthA = interthalamic adhesion.
Figure 2B shows the final electrode in the central thalamus visualized on a 3D atlas37. Two orthogonal planes of section along the axis of the electrode in the right hemisphere after registration of the 3D atlas with the CT scan by means of the atlas38. The four contacts of the electrode (blue circles) were located in the right thalamus (R-Thal). GPi = internal globus pallidus, STN = subthalamic nucleus, ZI = zona incerta, RPT = reticular perithalamic nucleus, RN = red nucleus.
Figure 2C shows a schematic drawing of the DBS electrode. Electrode contacts were re-referenced offline, resulting in three bipolar LFP channels for each hemisphere (LFPL01, LFPL12, LFPL23, LFPR01, LFPR12, and LFPR23). EEG electrode montage (10-20 system) with electrodes used during recording in the DOC case-example (Fz, Cz, Pz, Oz, T4, T3 and Fpz) (Figure 2D)
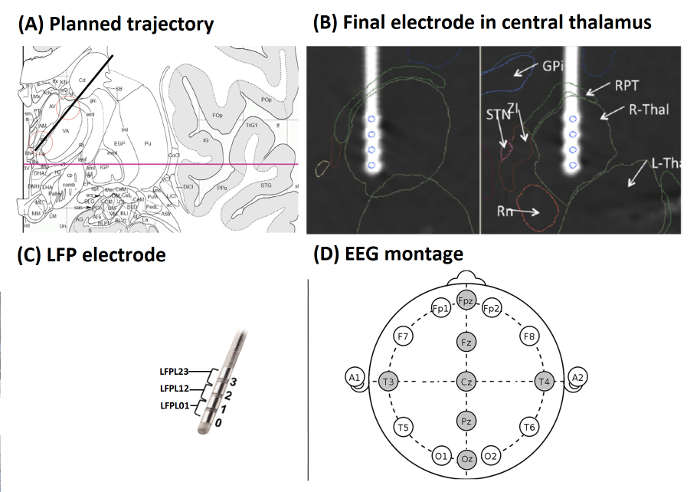
Figure 2: Target Localization, LFP Electrode and EEG Set-up (from Example 2). (A) Planned trajectory (black line) projected on an anatomic atlas36, section 30, coronary, 10.7 mm behind AC (red line: AC-PC plane). Red circles mark targeted areas of the lowermost 15 mm (atlas grid size: 10 mm) with iml = internal medullary lamina thalami and Rt = reticular thalamic nucleus. VA = ventroanterior thalamic nucleus, AV = anteroventral thalamic nucleus, AM = anteromedial thalamic nucleus, Fa = fasciculosus nucleus, IthA = interthalamic adhesion. (B) Final electrode in the central thalamus visualized on a 3D atlas37. Two orthogonal planes of section along the axis of the electrode in the right hemisphere after registration of the 3D atlas with the CT scan by means of an atlas38. The four contacts of the electrode (blue circles) were located in the right thalamus (R-Thal). GPi = internal globus pallidus, STN = subthalamic nucleus, ZI = zona incerta, RPT = reticular perithalamic nucleus, RN = red nucleus. (C) Schematic drawing of the DBS electrode. Electrode contacts were re-referenced offline, resulting in three bipolar LFP channels for each hemisphere. (D) EEG electrode montage (10 – 20 system) with electrodes used in the DOC case-example highlighted in gray. (Figures A and B were modified with permission from26, Figure C was modified with permission from Medtronic). Please click here to view a larger version of this figure.
Figure 3A shows exemplary EEG recordings corresponding to bipolar channels: T4Cz, T3Cz, PzCz, OzPz and FzPz in the case of the neutral non-addressing condition (left) and the familiar addressing condition (right).
Figure 3B displays exemplary LFP recordings corresponding to bipolar channels: LFPL23 and LFPR23 in the case of the non-addressing condition (left) and the familiar addressing condition (right).

Figure 3: Exemplary Recordings (from Example 2). (A) Figure shows EEG recordings.The figure illustrates EEG traces corresponding to bipolar channels (see 4.2 for details about channel re-referencing). (B) Figure shows LFP recordings.The figure illustrates LFP traces corresponding to bipolar channels in the case of left and right hemispheres (see 4.2 for details about channel re-referencing). Please click here to view a larger version of this figure.
Analysis of stimulus-locked modulation of oscillatory activity within central thalamus revealed a right-sided significant (p = 0.044) increase of beta power (12-25 Hz) within the first second (0.45-0.55 sec) when contrasting neutral addressing vs. familiar-addressing conditions (Figure 4A).
Coherence analysis between channels PzCz (EEG) and LFPR23 (right hemisphere) revealed a significant difference between conditions in the theta band. Also, the imaginary part of coherence showed deviation from zero indicating a phase delay between LFP and EEG (Figure 4B). Local analysis revealed significant (p = 0.01) theta-gamma PAC (with max. at 5-to-75 Hz) for the right local LFP channel (LFPR23-LFPR23) in the familiar-addressing condition (Figure 4C).
Analysis of power change corresponding to LFP23 revealed an early beta increase within the first second (green box) and a late theta modulation (red box) (Figure 4D, Top). It is also noticeable that Gamma around 40 Hz (green circle/ellipse) is followed by a broader and higher gamma up to 80 Hz (Figure 4D, Top). A significant theta increase in the familiar-addressing condition at 4-6.5 Hz and time period 2.6-2.8 sec (red circle), (p = 0.048) on LFPL23 as well as an increased trend on LFPR23 were revealed (Figure 4D, Bottom).
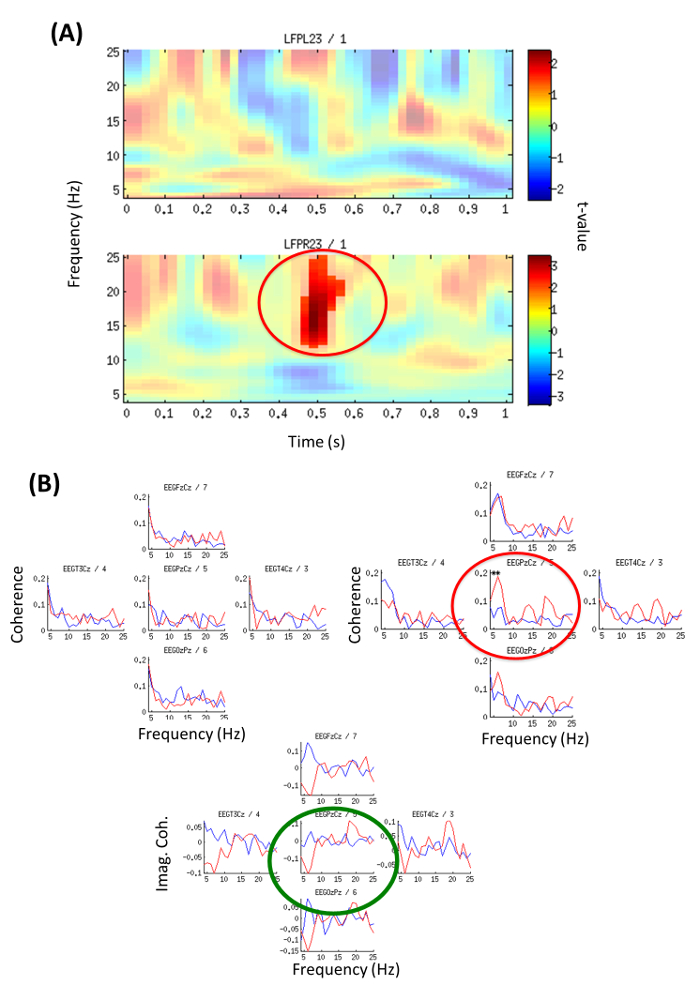
Figure 4: Time-frequency Power Analysis and EEG-LFP Coherence (from Example 2). (A) Local oscillatory power contrasting neutral versus familiar-addressing condition for the first second; Color code represents t-values. Top: left channel LFPL23; Bottom: right channel LFPR23. Significant beta increase (p = 0.044) at 12-25 Hz, 0.45-0.55 sec (red circle). (Modified with permission from26). (B) Familiar-addressing condition (red line) and neutral non-addressing condition (blue line). Coherence was calculated on independent 1 sec segments from epochs with duration 0-4 sec and averaged across all segments. Top (left): Coherence with channel LFPL23 left hemisphere, Top (right): Coherence with channel LFPR23 right hemisphere. Significant difference between conditions (p = 0.044) is indicated by red circle/stars for coherence with channel PzCz, 5-6 Hz. Bottom: Imaginary part of coherence between LFPR23 right hemisphere and channel Cz (green circle) shows deviation from zero meaning a phase delay between LFP and EEG (thus effect not due to volume conduction). (Modified with permission from26) Please click here to view a larger version of this figure.
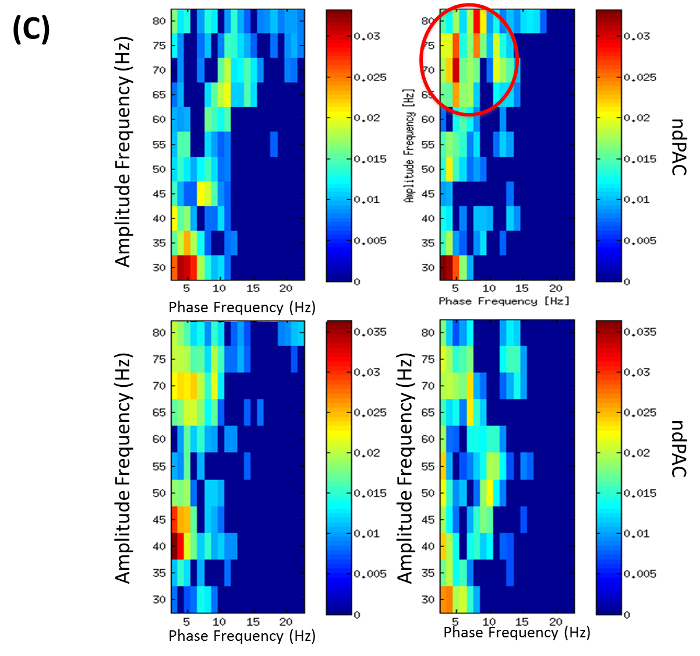
Figure 4C: Phase Amplitude Coupling (PAC) (from Example 2). PAC for phase frequencies 3-22 Hz and amplitude frequencies 35-80 Hz. Colors encode normalized direct phase-amplitude cross-frequency coupling (ndPAC). Spurious coupling is set to 0 (p = 0.01). Conditions: left: neutral, right: familiar-addressing. Top: PAC of right local LFP channel LFPR23-LFPR23 showing PAC in familiar addressing condition with max. at 5-75 Hz (red circle). Bottom: PAC of right LFP-EEG combination with LFPR23-EEGPzCz. (Modified with permission from26) Please click here to view a larger version of this figure.
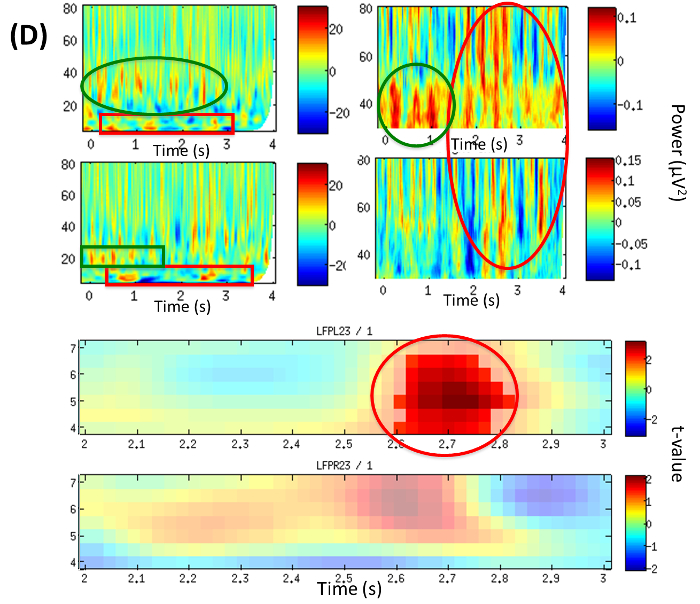
Figure 4D: LFP Time-frequency Analysis (from Example 2). Time frequency plots of local power changes at LFP23. TOP: Power difference from baseline in the familiar-addressing condition over the period of the trial (0-4 sec). Left: broad frequency band 5-80 Hz, right: gamma band; top row: left hemisphere (LFPL23), bottom row: right hemisphere (LFPR23). BOTTOM: Statistical contrast between conditions illustrating significant theta increase in the familiar-addressing condition at 4-6.5 Hz and time period 2.6-2.8 sec (red circle), p = 0.048 on LFPL23 and increase (trend) on LFPR23. Color map encodes t-values; top: left hemisphere (LFPL23), bottom: right hemisphere (LFPR23). (Modified with permission from26) Please click here to view a larger version of this figure.
