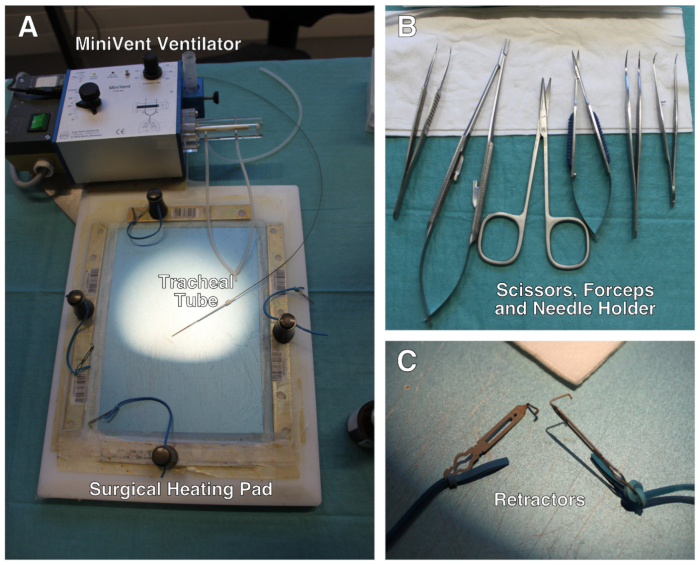
Figure 1: Description of the surgical setup. (A) Surgical setup comprises a modified heating pad, a ventilator and retractors attached to elastic bands. (B) Set of scissors, forceps and needle holder used during the surgery. (C) Close-up of the mini-retractors. Not shown: surgical stereomicroscope.
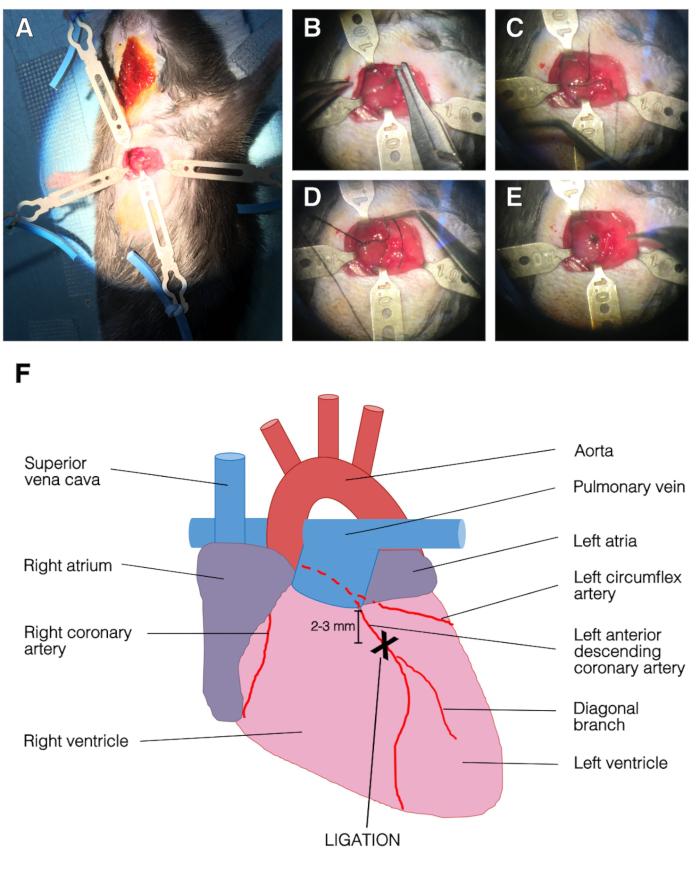
Figure 2: Representative images of the surgery and LAD ligation. (A) Opened chest with retractors. The left ventricle was apparent. Top, left and bottom retractors held the ribcage and right retractor held the pectoralis muscle. (B) The needle was passed under the LAD. (C) Suture silk was passed under the LAD, into the left ventricle. (D) Single stitch on the LAD. (E) End of the ligation procedure, the suture was secured with three knots. (F) Representation of an anterior view of the heart. The position of LAD ligation was 2-3 mm below left atria and above diagonal branch of the LAD.
