The comparison of procedure time between modified and traditional methods.
The procedure time from the beginning of cutting the skin to the end of closing skin was recorded in 5 mice with the modified approach and 5 mice with the traditional approach, respectively. A minimal number of animals was used to obtain results with statistical significance. Compared with the control of the traditional approach7,14 to perform SNIt, the modified approach took almost half the amount of procedure time (236.2 ± 28.6 s vs. 422.6 ± 53.8 s, p=0.0156; Figure 4).
The comparison of mechanical hypersensitivity between the two methods.
No difference of von Frey assessment (manual) was observed in the two groups at baseline (1.05 ± 0.10 g vs. 0.96 ± 0.13 g, p=0.9405). Compared with the traditional method (n=9), the modified method (n=14) induced similar mechanical hypersensitivity on the ipsilateral side from post-operative day 1 to post-operative day 14 (0.33 ± 0.09 g vs. 0.32 ± 0.05 g, p>0.9999, at post-operative day 1; 0.19 ± 0.02 g vs. 0.27 ± 0.06 g, p=0.9485 , at post-operative day 3; 0.20 ± 0.06 g vs. 0.15 ± 0.05 g, p=0.9979, at post-operative day 5; 0.13 ± 0.02 g vs. 0.15 ± 0.03 g, p>0.9999, at post-operative day 7; and 0.14 ± 0.02 g vs. 0.19 ± 0.03 g, p=0.9937, at post-operative day 14; Figure 5A).
Compared with percentage response between traditional (n=5) and modified method (n=5), similar mechanical hypersensitivity was observed on the ipsilateral side from baseline (4.00% ± 2.45% vs. 6.00% ± 2.45%, p>0.9999) to post-operative day 1 (20.00% ± 3.16% vs. 12.00% ± 3.74%, p=0.8987), day 3 (30.00% ± 5.48% vs. 32.00% ± 4.90%, p>0.9999), day 5 (36.00% ± 9.27% vs. 30.00% ± 5.48%, p=0.9730), day 7 (32.00% ± 8.00% vs. 36.00% ± 4.00%, p=0.9968), and day 14 (38.00% ± 5.83% vs. 36.00% ± 7.48%, p>0.9999; Figure 5B).
No neural reconnection between the distal and remaining stump at post-operative day 14.
Because the axon regeneration proceeds at a rate of 1-3 mm/d15, whether there is nerve regeneration at post-operative day 14 should be taken into account. On the post-operative day 14, the modified SNI mice were perfused intracardially with 0.1 mol/L phosphate-buffered saline followed by a phosphate-buffered 10% formalin fixative, and the nerve ligation site was dissected and exposed. No neural reconnection was observed between the distal and remaining stumps (Figure 3D).

Figure 1. Illustration of the 3 branches of the sciatic nerve that are separated at the superior edge of the gastrocnemius muscle (GM) around the knee area. The tibial nerve runs under the GM muscle, and the common peroneal nerve and sural nerve run above the GM muscle. 1: sciatic nerve; 2: tibial nerve; 3: common peroneal nerve; 4: sural nerve. Abbreviations: BFM = biceps femoris muscle; GM = gastrocnemius muscle. Please click here to view a larger version of this figure.
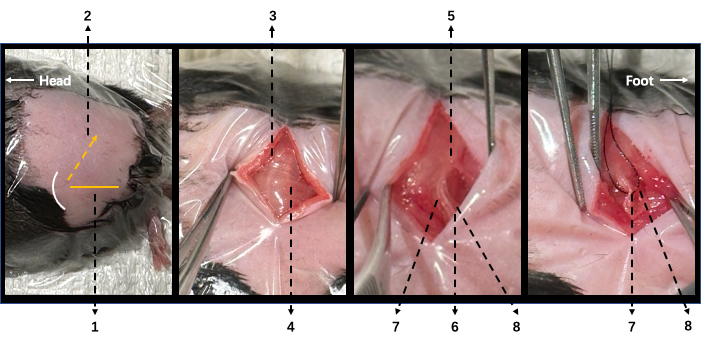
Figure 2. Illustration of surgical procedure in modified SNI mice. (A) In a lateral position, the left leg is upside with knee flexion. The yellow horizontal line (1) indicates the horizontal line crossing the knee level, and the yellow dashed arrow (2) indicates the incision. (B) Following a skin incision, two white lines can be visualized under the biceps femoris muscle (BFM). The femur is under the cephalad one (3), and the sciatic nerve is under the caudal one (4). (C) After careful dissection of BFM, the sciatic nerve (5) and its three branches can be visualized: the tibial (6), common peroneal (7), and sural (8) nerves. (D) The common peroneal (7) and sural (8) nerves were ligated together. 1: horizontal line crossing knee; 2: cut incision; 3: femur on the underneath; 4: sciatic nerve on the underneath; 5: sciatic nerve; 6: tibial nerve; 7: common peroneal nerve; 8: sural nerve; 9: white curve line indicates knee. Please click here to view a larger version of this figure.

Figure 3. Illustration of sciatic, tibial, sural, and common peroneal nerves with the ligation of modified SNI in intracardially perfused mice. (A) Sciatic nerve (1) and its three branches: the tibial nerve (2) passing under the gastrocnemius muscle (5), and the common peroneal (3) and the sural (4) nerves running above the gastrocnemius muscle. (B) Suture needle crossing under common peroneal and sural nerves together. (C) A 6-0 nylon suture was used for the ligation of common peroneal and sural nerves together. (D) No reconnection between distal and remaining nerve stump at post-operative day 14 was observed. 1: sciatic nerve; 2: common peroneal nerve 3: tibial nerve; 4: sural nerve; 5: gastrocnemius muscle; 6: ligation. Please click here to view a larger version of this figure.

Figure 4. The modified method is faster than the traditional SNI method to perform. Compared to the traditional SNI method (n=5), the modified method (n=5) requires much less procedure time to perform. Analyses were performed using an unpaired t-test, and data are presented as mean ± SEM. Please click here to view a larger version of this figure.

Figure 5. von Frey assessment of mechanical responsiveness in traditional and modified SNI models. (A) The modified SNI (n=9) and traditional SNI (n=14) models induced similar mechanical hypersensitivity on the ipsilateral side in 14-day follow-up. (B) The modified SNI (n=5) and traditional SNI (n=5) models acquired similar percentage responses on the ipsilateral side in a 14-day follow-up. Analyses were performed using two-way ANOVA with Sidak's multiple comparisons test. Data are presented as mean ± SEM. Please click here to view a larger version of this figure.
