Mice were euthanized seven days after surgery. Animals were anesthetized with 80 mg/kg ketamine and 10 mg/kg xylazine. Under anesthesia, blood was drawn from vena cava and heart was sampled. Atria were removed, myocardium were washed in ice-cold PBS. For measurements of ischemic areas, hearts were frozen at -20 °C for 40 min, then sliced and stained for 20 min at 37 °C in PBS containing 2% triphenyltetrazolium chloride (TTC). Heart slices were fixed overnight in 4% buffered paraformaldehyde solution at room temperature. Ischemic areas remained unstained whereas live tissue was stained in red due to the presence of dehydrogenases. Ischemic areas were calculated as percentage of white area of the left ventricle (LV) with an imaging software (Figure 3A, B). For biochemical and molecular biology analyses, hearts were frozen in liquid nitrogen. After grinding hearts on liquid nitrogen the organ powder was used for protein and mRNA extraction. The extent of fibrosis in the myocardial tissue of infarcted hearts was assessed by western blot analysis of alpha smooth-muscle actin (αSMA) and SMAD2 phosphorylation, which are respectively major read-outs of myofibroblasts and of TGFβ signaling activation (Figure 3C). mRNA expression of Tgfb, and downstream targets Ctgf, Postn and Il11 are all indicators of myocardial fibrosis. This was shown by real-time polymerase chain reaction (PCR) analysis (Figure 3D).
Pro-inflammatory signaling pathways and expression of pro-inflammatory genes were typically found activated within the first week following myocardial infarction. Phosphorylation of NF-κB p65 transcription factor is a hallmark of inflammation and was observed in whole myocardium extracts of the MI mice (Figure 3E). mRNA expression of pro-inflammatory genes Il1b, Il6 and Cxcl10 (Figure 3F) and monocytes/macrophages markers Cd14 and Mertk were analyzed by real-time PCR (Figure 3G). Note that there was a variability in the extent of NF-κB p65 and SMAD2 phosphorylation (Figure 3C,E, lanes 4-7). This variability depends largely on the size of the infarct.
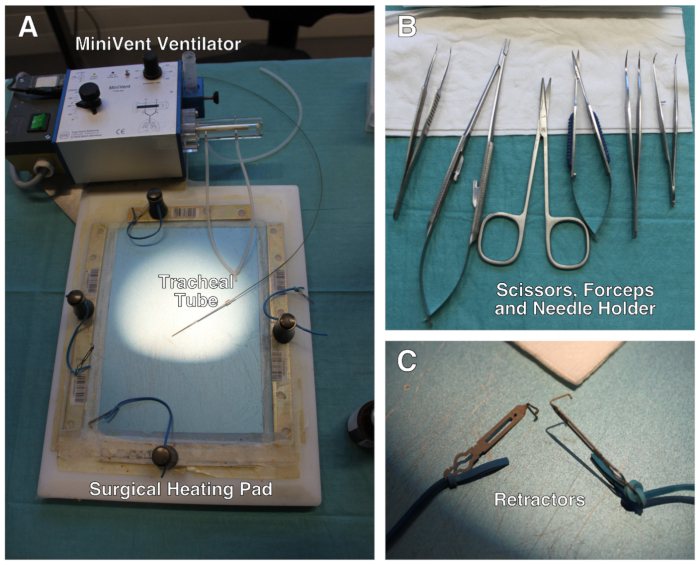
Figure 1: Description of the surgical setup. (A) Surgical setup comprises a modified heating pad, a ventilator and retractors attached to elastic bands. (B) Set of scissors, forceps and needle holder used during the surgery. (C) Close-up of the mini-retractors. Not shown: surgical stereo microscope. Please click here to view a larger version of this figure.
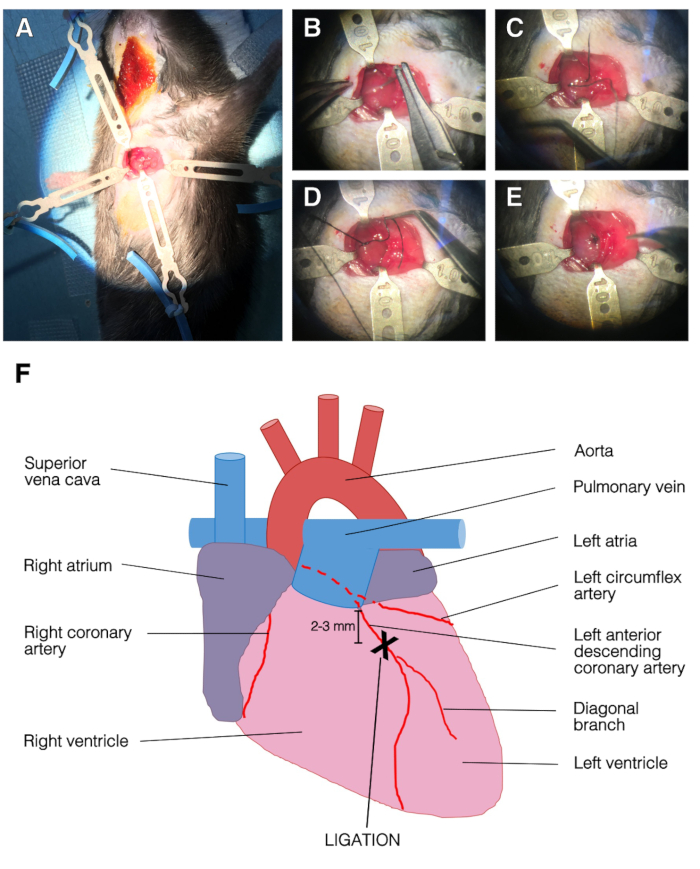
Figure 2: Representative images of the surgery and LAD ligation. (A) Opened chest with retractors. The left ventricle was apparent. Top, left and bottom retractors held the ribcage and right retractor held the pectoralis muscle. (B) The needle was passed under the LAD. (C) Suture silk was passed under the LAD, into the left ventricle. (D) Single stitch on the LAD. (E) End of the ligation procedure, the suture was secured with three knots. (F) Representation of an anterior view of the heart. The position of LAD ligation was 2-3 mm below left atria and above diagonal branch of the LAD. Please click here to view a larger version of this figure.
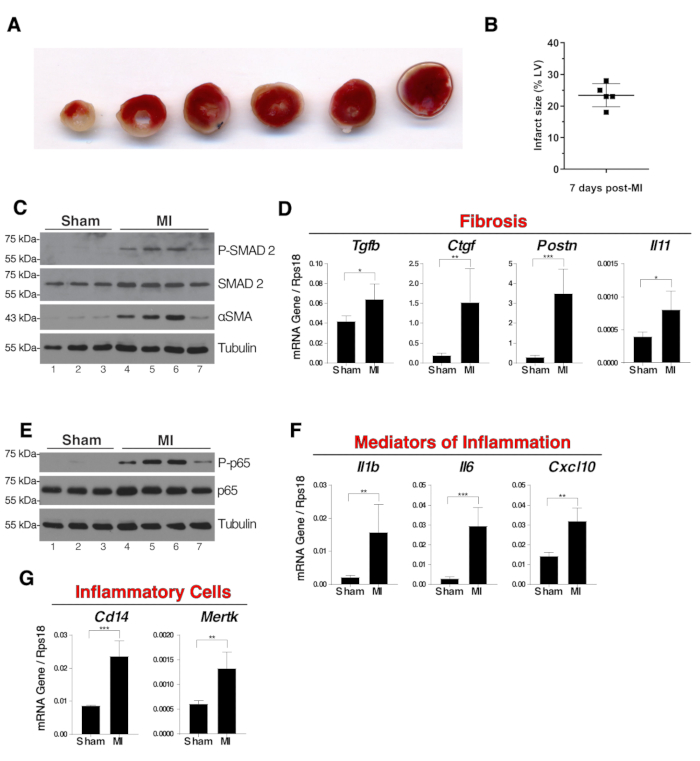
Figure 3: Fibrosis and inflammation in whole myocardium extracts seven days post-surgery. (A) Representative images of TTC staining of a sliced infarcted heart seven days post-surgery. Pale ischemic areas remained unstained and white whereas live tissue was stained red. The ligation was visible on the third slice from the left. (B) The size of the ischemic areas of five infarcted hearts were measured using TTC staining technique. Results were the percentage of white area of the left ventricle (LV). (C) Western blot analysis of SMAD2 phosphorylation and alpha-SMA expression in whole myocardium as indicators of fibrosis. (D) mRNA expression of Tgfb, Ctgf, Postn and Il11 in whole myocardium extracts. (E) Western blot of NF-κB p65 phosphorylation in whole myocardium extracts. (F) mRNA expression of pro-inflammatory genes Il1b, Il6 and Cxcl10 in whole myocardium extracts. (G) mRNA expression of Cd14 and Mertk as indicators of the presence in the myocardium of monocytes/macrophages and phagocytic macrophages respectively. N = 3 in sham and N = 4 in MI group. For mRNA expression analysis, expression was relative to the endogenous control Rps18 and group comparisons were unpaired Student's T-tests, *p ≤ 0.05, **p ≤ 0.01, *** p ≤ 0.001. In panels B, D, F and G error bars represent standard deviations. Please click here to view a larger version of this figure.
