Figure 2 shows a typical view of an aEEG monitor. Continuous and discontinuous normal voltage patterns are considered physiological background patterns in term and preterm infants, respectively (Figure 3 and Figure 4). A burst suppression pattern, continuous low-voltage pattern, and a flat trace are pathological background patterns (Figure 5, Figure 6, Figure 7).
Seizures in term infants have a characteristic shape, with a sudden rise of both the lower and upper border (Figure 8). In preterm infants, however, seizures can be camouflaged by the discontinuous pattern and may only be detected by viewing the raw EEG (Figure 9).
Liquid bridging can cause an apparent flat trace (Figure 10). Usually, this happens in the two-channel aEEG (intraparietal curves). If the cross-cerebral aEEG is physiological, while the intraparietal curve shows a flat trace, the electrodes should be checked for liquids. Electrical interference, movements, and handling can lead to an apparent seizure or even to an apparent status epilepticus. If this happens, impedance and the reference electrode should be checked, and the raw EEG should be viewed (Figure 11). Another reason for an elevation of both the lower and upper border is the displacement of the reference electrode.

Figure 1. Formation of the aEEG Tracing.
The signal from the raw EEG (upper curve) is processed, resulting in the amplitude-integrated EEG band (lower curve). High amplitudes form the upper border, whereas low amplitudes form the lower border. While strong variation in the height of the amplitude leads to a broad aEEG band, the aEEG band is narrow if there is little variation in the height of amplitude. The scale of the y-axis is linear up to 10 µV and logarithmic above 10 µV. Please click here to view a larger version of this figure.
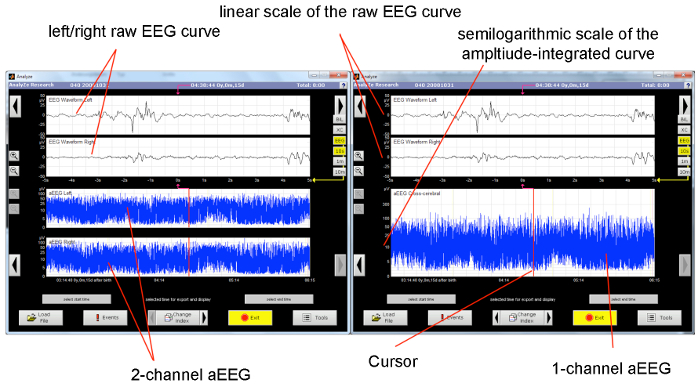
Figure 2. Typical Display of an aEEG Monitor.
The upper half of the monitor displays the raw EEG curve (the displayed section equals 10 s). On the left display, the lower half shows the unilateral aEEG tracing (the displayed section equals approximately 3 h). On the right display, the corresponding cross-cerebral tracing is shown. The cursor indicates the section of the amplitude-integrated tracing from the raw EEG. Please click here to view a larger version of this figure.

Figure 3. Continuous Normal Voltage Pattern.
Continuous background pattern with sleep-wake cycling. The x-axis equals time (one square = 10 min). Please click here to view a larger version of this figure.
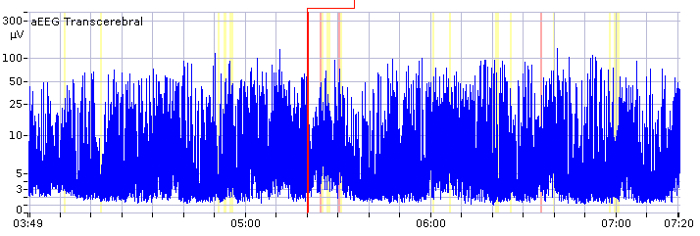
Figure 4. Discontinuous Normal Voltage Pattern.
Discontinuous background pattern with imminent sleep-wake cycling. The x-axis equals time (one square = 10 min). Please click here to view a larger version of this figure.

Figure 5. Burst Suppression Pattern.
Burst suppression pattern, with the lower amplitude continuously low and without alteration. The x-axis equals time (one square = 10 min).
From Bruns, N. Amplituden-integriertes EEG bei extrem unreifen Frühgeborenen in den ersten 4 Lebenswochen. http://www.diss.fu-berlin.de/diss/receive/FUDISS_thesis_000000036576 (2012). Please click here to view a larger version of this figure.
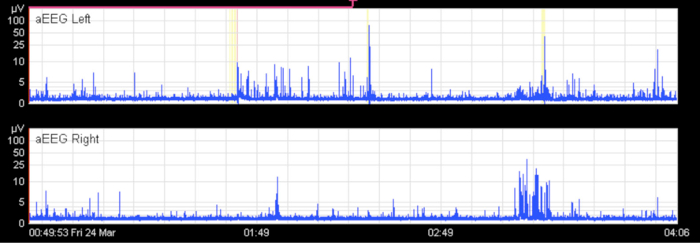
Figure 6. Flat Trace.
Flat trace on both sides in a term infant with severe meningoencephalitis. The x-axis equals time (one square = 10 min).
From Bruns, N. Amplituden-integriertes EEG bei extrem unreifen Frühgeborenen in den ersten 4 Lebenswochen. http://www.diss.fu-berlin.de/diss/receive/FUDISS_thesis_000000036576 (2012). Please click here to view a larger version of this figure.

Figure 7. Continuous Low-voltage Pattern.
Continuous low-voltage pattern without sleep-wake cycling. The x-axis equals time (one square = 10 min).
From Bruns, N. Amplituden-integriertes EEG bei extrem unreifen Frühgeborenen in den ersten 4 Lebenswochen. http://www.diss.fu-berlin.de/diss/receive/FUDISS_thesis_000000036576 (2012). Please click here to view a larger version of this figure.

Figure 8. Seizures in Term Infants.
Typical depiction of a seizure in the aEEG: a sudden rise of the lower and upper margin is followed by a short period of decreased activity. Repetitive seizures for approximately 3.5 h. The x-axis equals time (one square = 10 min).
From Bruns, N. Amplituden-integriertes EEG bei extrem unreifen Frühgeborenen in den ersten 4 Lebenswochen. http://www.diss.fu-berlin.de/diss/receive/FUDISS_thesis_000000036576 (2012). Please click here to view a larger version of this figure.
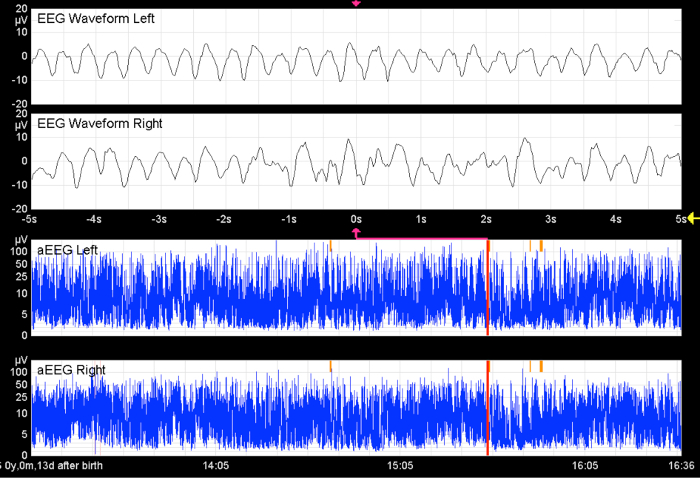
Figure 9. Seizures in Preterm Infants.
Without the raw EEG, the hypersynchronous activity in both hemispheres would remain undetected. The x-axis equals time (one square = 10 min).
From Bruns, N. Amplituden-integriertes EEG bei extrem unreifen Frühgeborenen in den ersten 4 Lebenswochen. http://www.diss.fu-berlin.de/diss/receive/FUDISS_thesis_000000036576 (2012). Please click here to view a larger version of this figure.
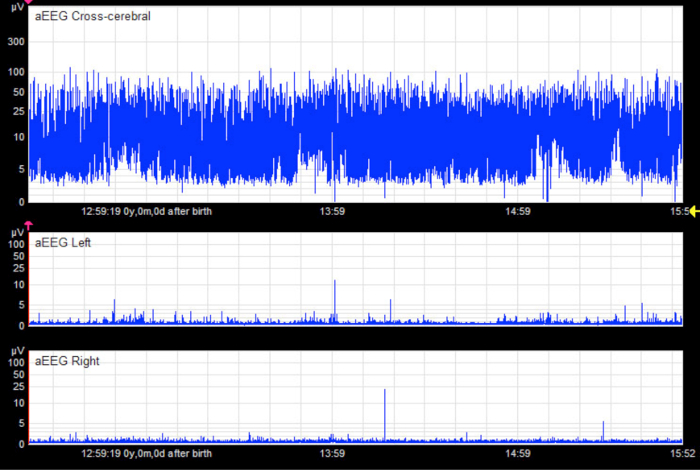
Figure 10. Apparent Flat Trace.
In the unilateral tracings, there appears to be a pathological flat trace pattern in an infant without cerebral injury. The cross-cerebral tracing shows a physiological discontinuous background pattern with short sections of continuous activity. In this case, the flat trace is an artifact caused by liquid bridging between electrodes (especially hydrogel electrodes). The x-axis equals time (one square = 10 min).
From Bruns, N. Amplituden-integriertes EEG bei extrem unreifen Frühgeborenen in den ersten 4 Lebenswochen. http://www.diss.fu-berlin.de/diss/receive/FUDISS_thesis_000000036576 (2012). Please click here to view a larger version of this figure.
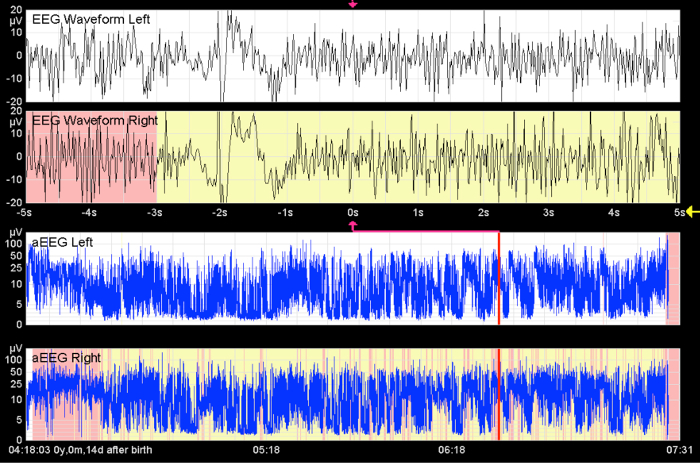
Figure 11. Apparent Seizures.
This image shows high-frequency activity over a long period of time. Without seeing the raw EEG curve, status epilepticus is indicated. This artifact is caused by muscle activity. The x-axis equals time (one square = 10 min).
From Bruns, N. Amplituden-integriertes EEG bei extrem unreifen Frühgeborenen in den ersten 4 Lebenswochen. http://www.diss.fu-berlin.de/diss/receive/FUDISS_thesis_000000036576 (2012). Please click here to view a larger version of this figure.
