We tested the effects of air bubble contamination in an LFPI device on waveform formation. We injected air bubbles into the device and compared the oscilloscope outputs with oscilloscope data collected from a non-contaminated LFPI device. Conditions were as follows: non-contaminated, injection of 5 mL of air, injection of 10 mL of air, and injection of 15 mL of air. We kept the pendulum at a consistent height for all impacts for all conditions, and we performed 15 impacts per condition.
When performing an injury or testing the LFPI device, the pressure waveform on the oscilloscope should show a single, sharp peak (Figure 2A). The presence of air bubbles in the device will result in a waveform with several short peaks (Figure 2B), indicating bubbles that need to be removed. After reassembling the device, and before any injury session, we also recommend performing four to five test drops (no mouse attached) with the pendulum to ensure that the device is performing repeatably. In addition to irregularities in the pressure waveform, behavioral changes after injury/sham LFPI can also be indicative of whether the device is functioning properly. Injured mice should have prolonged righting reflex times after LFPI in comparison to sham mice, and these times should be monitored and recorded. Righting times that are either too long or too short may be an indication of improper device assembly and/or cleaning15. Similar symptoms can also appear gradually in a device that has been properly cleaned and filled (likely due to the slow accumulation of bubbles during routine use), indicating that it is time to repeat the cleaning and refilling. Scheduling preventive maintenance once every 6 months can help to ensure consistent performance of the LFPI device.
As seen in Table 1, the presence of air bubbles changed the voltage of the waveform when compared to a fully filled, non-contaminated LFPI device. Increasing the size of the air bubble gradually decreased the voltage of the wave, as indicated by the oscilloscope outputs.
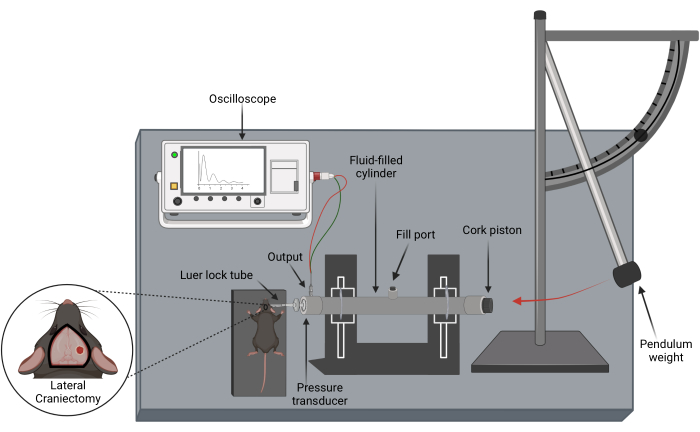
Figure 1: Schematic of the LFPI device and lateral craniectomy performed prior to injury. This device is used to reproduce TBIs with no skull fracture in animal models by causing displacement and/or deformation of the brain due to an increase in intercranial pressure. Created with Biorender.com. Please click here to view a larger version of this figure.

Figure 2: Monitoring pressure transducer output to assess LFPI device maintenance and functional status13. (A) Representative image of the pressure waveform produced by a properly cleaned and functioning LFPI device. (B) Sample image of a pressure waveform indicating the presence of air bubble contamination. Please click here to view a larger version of this figure.
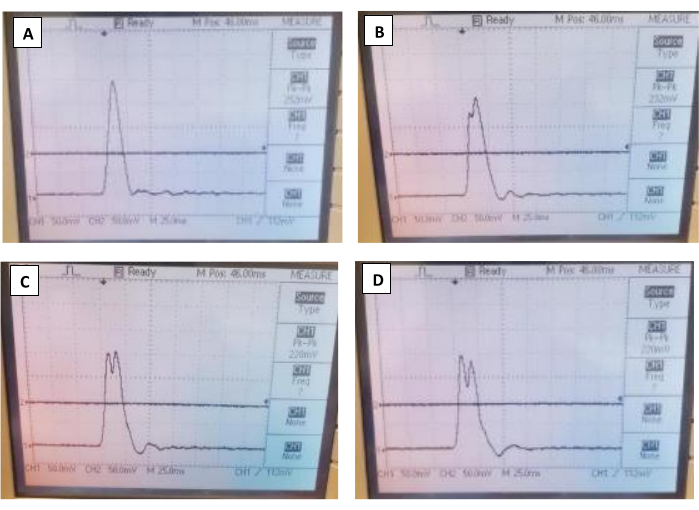
Figure 3: Representative image of oscilloscope outputs for all four conditions. (A,B,C,D) The oscilloscope outputs for the non-contaminated, 5 mL of air injection, 10 mL of air injection, and 15 mL of air injection, respectively. Please click here to view a larger version of this figure.
| Air Bubble Contamination Condition | |||||
| Filled and Non-Contaminated LFPI Device | 5 mL of Total Air Injected | 10 mL of Total Air Injected | 15 mL of Total Air Injected | ||
| Waveform Output (mV) | 240 | 218 | 230 | 218 | |
| 234 | 222 | 226 | 220 | ||
| 240 | 228 | 226 | 220 | ||
| 244 | 226 | 228 | 218 | ||
| 246 | 228 | 230 | 218 | ||
| 248 | 232 | 226 | 220 | ||
| 248 | 230 | 226 | 220 | ||
| 250 | 230 | 228 | 220 | ||
| 248 | 232 | 228 | 224 | ||
| 252 | 232 | 228 | 222 | ||
| 250 | 232 | 226 | 220 | ||
| 250 | 230 | 228 | 222 | ||
| 252 | 230 | 228 | 222 | ||
| 252 | 232 | 228 | 220 | ||
| Average Waveform Output (mV) | 246.7 | 228.7 | 227.6 | 220.3 | |
Table 1: Oscilloscope voltage outputs from non-contaminated control group compared to contaminated conditions. Paired t-tests were performed between the non-contaminated conditions and each contaminated condition. All contaminated conditions were significantly decreased when compared to non-contaminated conditions (p < 0.0001).
