Herein, we introduce the robot-assisted rehabilitation that our group is currently working on: the biofeedback effects on upper limb motor deficit in patients with acute stroke. We included 10 consenting stroke patients (mean age: 66.8 ± 12.0 years; two women and eight men) who were admitted to our hospital. At the subacute stroke stage, more than 2 weeks after the onset, we evaluated the motor-related cortical activity of these patients using an fNIRS system before and immediately after upper limb robot-assisted rehabilitation on the same day. Regarding the block design tasks, they carried out affected elbow flexion/extension movements 15x within 15 s in each task cycle, and they repeated seven task cycles. In addition, six healthy volunteers (mean age: 58.7 ± 7.1 years; two women and four men) were also enrolled as controls to identify the location of the normal task-related cortical activation during the right elbow flexion/extension movements.
Figure 5 shows the results of the group analysis of 10 stroke patients by the t-statistical mapping values using GLM models with the NIRS-SPM software. This method showed an increase in the cortical activity of the primary motor cortex in the measured hemisphere immediately after the robot-assisted rehabilitation compared with that before the training. The pre-intervention data gathering, intervention (robot-assisted exercise), and the post-intervention data gathering were performed at the single experimental session on the same day and at the same place.
Figure 6 shows the results of the multi-channel group analysis comparing pre- versus post-intervention (robot-assisted exercise). Statistical analysis of the multi-level hierarchical mixed model with the SAS software was performed. Increased cortical activity in the primary motor cortex was observed after intervention, the same brain region as in the NIRS-SPM.
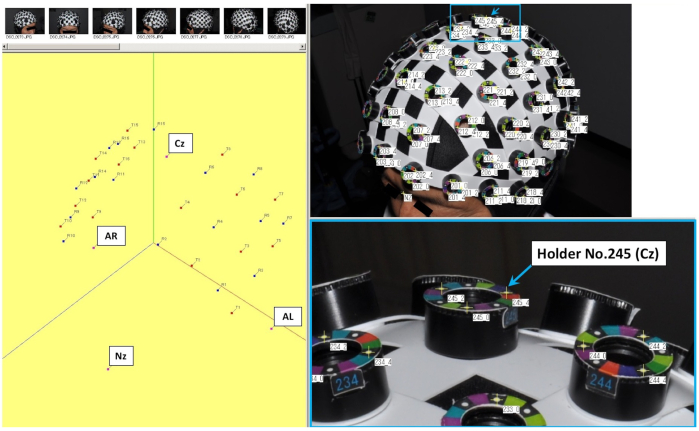
Figure 1: Setting of three-dimensional (3D) spatial registration and each holder of the head cap used for fNIRS recording. The No. 245 holder indicated by the arrow in the figure shows the central position (Cz), which is one of the coordinate axes. Please click here to view a larger version of this figure.

Figure 2: Arrangement of the 48-channel system with 32 optodes during the fNIRS recording. (A) Location of probes on head holder, (B) arrangement of the 48 channels and probes (16 light sources and 16 detectors; 4 x 4 array for each hemisphere) to a head cap bilaterally over the cortical areas, as regions of interest. Please click here to view a larger version of this figure.
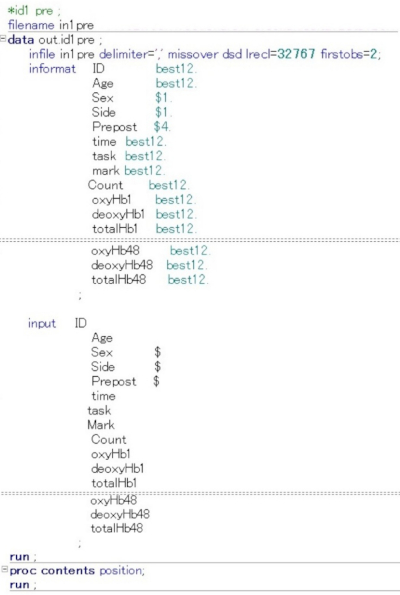
Figure 3: Command input for creating files used in the SAS analysis software. The figure shows how to define terms and numerical values on the command input screen that converts the text file information obtained from the NIRS file into an Excel CSV file and then converts it for SAS analysis. ID, Age, Sex, ipsilesional side, before and after the intervention, total time, and task periods, were entered numerically. In addition, information on HbO2, HHb, and total hemoglobin concentration level (mM x mm) were also entered. Please click here to view a larger version of this figure.

Figure 4: Command input used for each channel analysis in the SAS analysis software. In this multi-level hierarchical mixed model, the following numerical values were set and entered on the SAS command input screen. The status at rest (task = 0) and at task (task = 1) were compared, and the status at recovery (task = 2) was excluded. Furthermore, the status before the intervention was set to n = 0 and the status immediately after the intervention was set to n = 1, and the interaction was investigated for statistically significant differences in the amount of change in HbO2 and HHb for each channel. In the figure, the input screen information up to ch2 or ch47 is omitted. Please click here to view a larger version of this figure.
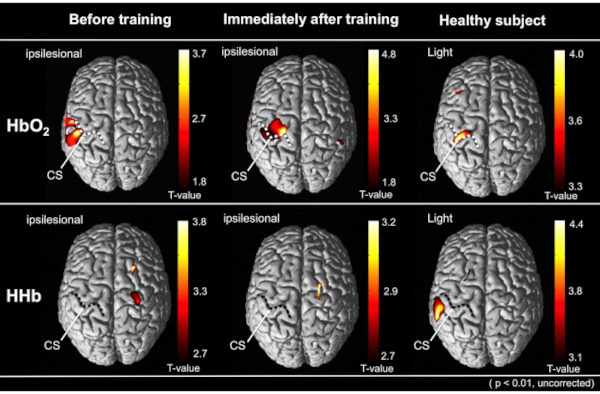
Figure 5: The results of the group analysis by the t-statistical mapping values using GLM models with the NRS-SPM software. The average cortical activity from all patients is depicted on the above view of the standardized brain models. The upper and lower represents the cortical activation in HbO2 and HHb level, respectively. The right image indicates the cortical activity of healthy subjects during the tasks. Comparing the robot-assisted rehabilitation before, the cortical activity was increased immediately after robot-assisted training on the same day. Compared to other cortical regions, each performing status was significantly increased (uncorrected, p < 0.01). Dotted lines indicate the central sulcus (CS) on the normalized brain images. This figure has been modified from Saita et al.15. Please click here to view a larger version of this figure.
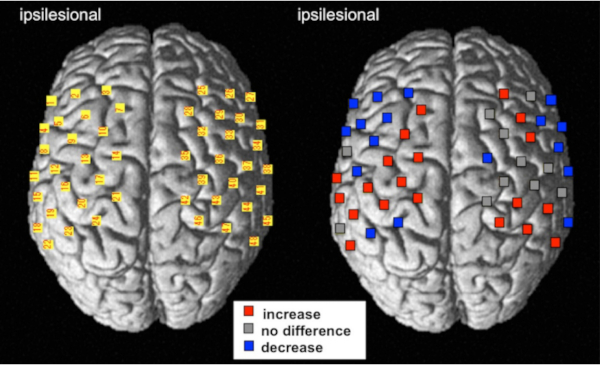
Figure 6: The result of the multi-channel analysis using multi-level hierarchical mixed models with the SAS software. The cortical activity of change represents the comparison between pre-and post-intervention using robot-assisted rehabilitation treatments. For the left image, the numbers of NIRS channels were superimposed on the standardized brain according to the MNI coordinate system. For the right image, red and blue indicate an increase and decrease in the HbO2 level, respectively (FDR corrected, p < 0.01). Gray indicates that the channels did not significantly change following the robot-assisted rehabilitation. This figure has been modified from Saita et al.15. Please click here to view a larger version of this figure.
