The optical mapping experiments are performed using the devices as shown in Figure 1a. The schema of the optical system is illustrated in Figure 1b. The system provides a high-resolution analysis of the membrane potential and Ca2+ transient in the atrium.
As depicted in Figure 1c and d, the isolated heart is positioned in a temperature-controlled chamber. A 1-French size electrode catheter is placed in the RA through a PE tube inserted into the SVC, and another indwelling PE tube is inserted into the LV cavity from the LV apex to avoid excessive pressure on the heart chamber. For a simultaneous ECG recording, the cathode (ECG lead [-]) is connected to the cannulation needle, and the anode (ECG lead [+]) is connected to the pin electrode inserted into the ventricular apex. The feature of this assembly is to avoid any mechanical damage to the atria.
For the evaluation of the membrane voltage, fluorescence using di-4-ANEPPS is recorded with up to a 10,000 frames/s sampling rate (Figure 2). The activation map is obtained during constant pacing delivered from the RA. The fine mapping enables the analysis of the detailed conduction pattern in small murine atria.
Figure 3 illustrates representative traces of the membrane voltages and Ca2+ transient in the LA using RH237 and Rhod2AM during constant pacing from the RA. We reduce the sampling rate of the mapping to 1000 frames/s to obtain a sufficient signal/noise ratio of the Rhod2AM signal with the present setting. However, the system provides a sufficient quality for analyzing the relationship between the action potential and Ca2+ transient.
We then perform an induction of an atrial tachyarrhythmia with programmed stimulation using mice under a pathological condition. Figure 4 exhibits an optical recording of an induced AT in a murine atrium stained with di-4-ANEPPS. The mouse undergoes a transverse aortic constriction procedure to apply a pressure overload to the atrium 10 days before the experiment6. We induce AT by triple extrastimuli pacing (120/100/100/80), and observe the propagation of the reentrant circuit.
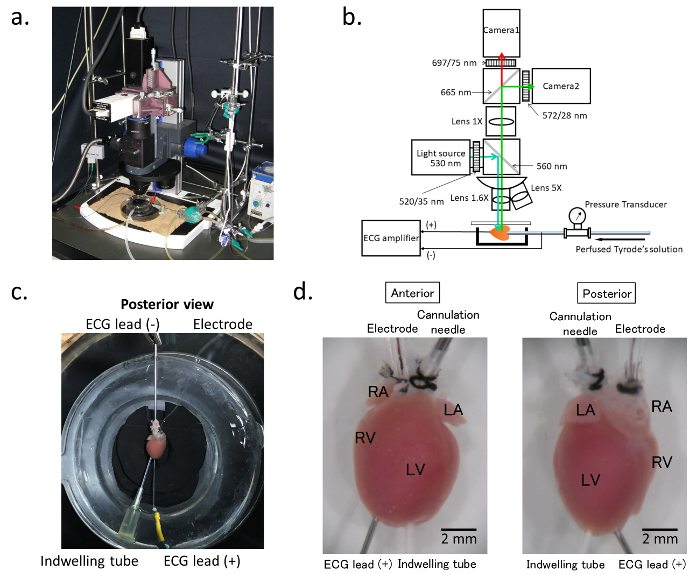
Figure 1. Optical mapping system. a. General assembly of the electrophysiology/optical mapping system. b. Schematic of the composition of the optical mapping system: The blue arrow indicates the excitation light generated by the light source. The objective lens can be exchanged with the turret. The emitted light from the stained heart is split between camera 1 and camera 2. Camera 1 detects the long wavelength signals for the membrane voltage, and camera 2 records the wavelengths with a bandpass filter of 580 ± 20 nm for the Ca2+ transient. During the procedure, the ECG and perfusion pressure are continuously recorded, and the ECG signal is also simultaneously imported into the optical map recording software. c. Preparation of the isolated hearts: The hearts are cannulated with a blunted needle via the ascending aorta for perfusion. For simultaneous ECG recordings, the cathode is connected to the cannulation needle, and the anode with the pin electrode is inserted into the ventricular apex. d. Cannulation tube and the electrodes: The heart is cannulated with a 21-gauge blunted needle for perfusion (cannulation needle). A 1-French size stimulating electrode (Electrode) is placed in the right atrium through a polyethylene tube inserted into the superior vena cava. The glass chamber is warmed at 37 ˚C by heated water circulating in the cavity of the chamber. Please click here to view a larger version of this figure.
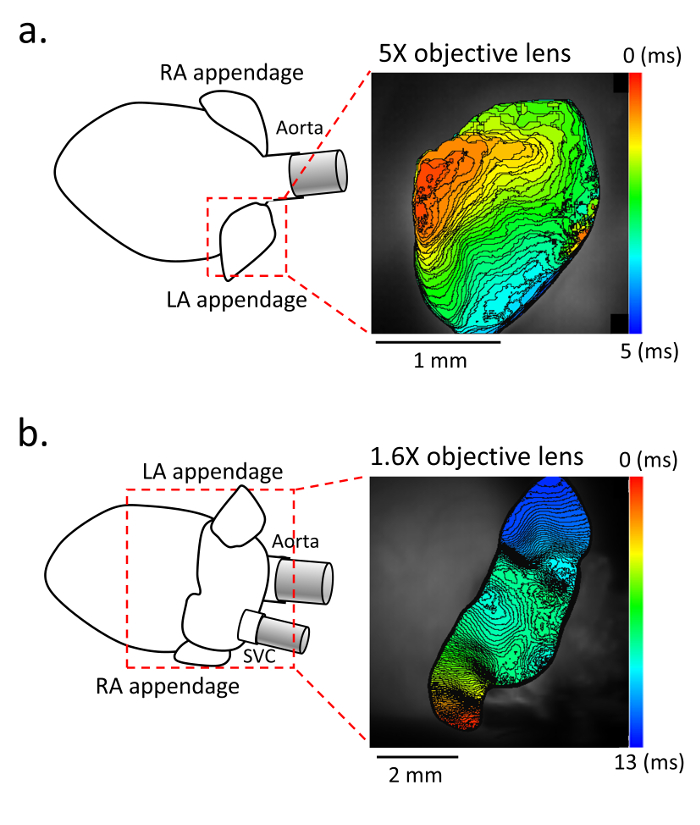
Figure 2. Activation map in the atrium. a. Representative activation maps in the anterior view with a 5X objective lens, and b. in the posterior view with a 1.6X objective lens. (Left panel) Schematic of the isolated heart and atrium. (Right panel) Activation map of the left atrium obtained with di-4-ANEPPS staining at 10,000 frames/s. The recording is performed under constant pacing with the stimulating electrode placed in the right atrium. Please click here to view a larger version of this figure.

Figure 3. Dual recording of the action potential and Ca2+ transient in the left atrium. a. Schematic of the isolated heart. b. Representative image of the intensity of the fluorescence in the left atrium using RH237 for the membrane voltage (Vm) and Rhod2AM for the Ca2+ transient. The recording is performed with a 5X objective lens at 1,000 frames/s. c. Simultaneous recording of the ECG (top), RH237 signal (middle), and Rhod2AM signal (bottom), during constant pacing with the stimulation electrode in the right atrium. The black arrows indicate the stimulation spikes, and yellow arrows the ventricular excitation. A light scattering effect from the ventricle also can be observed (yellow arrowheads) both in the RH237 signal and Rhod2AM signal. d. A merged RH237 and Rhod2AM trace. The action potential and transient Ca2+ changes are simultaneously recorded. Please click here to view a larger version of this figure.
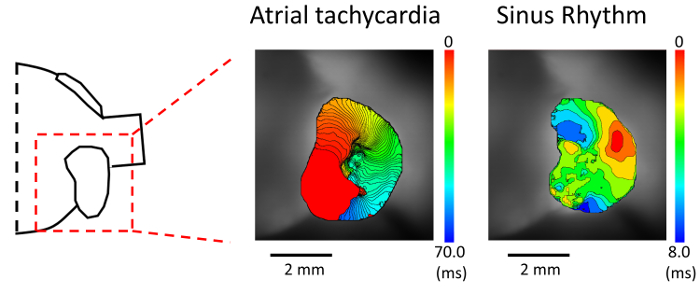
Figure 4. Activation mapping during atrial tachycardia. (Left panel) Schematic of the isolated heart. (Middle panel) Activation map during an atrial tachycardia (AT). AT was induced by triple extrastimuli pacing delivered from the right atrium. (Right panel) Activation map during sinus rhythm in the same mouse heart. Please click here to view a larger version of this figure.
Supplementary movie 1. Representative movie of the membrane potential in the atrium using staining with di-4-ANEPPS. Please click here to download this file.
Supplementary movie 2. Representative movies of the activation mapping during atrial tachycardia and sinus rhythm. Please click here to download this file.
