Diffusion Tensor Imaging—DTI—is a technique within magnetic resonance that relies on the diffusion of water molecules to study the integrity of white matter networks—the axon bundles that connect cortical and subcortical gray matter—in the brain.
These interconnecting structures can be damaged when an external force, such as a soccer ball, comes into contact with the head during a match. Such repetitive interactions can lead to more severe injury, referred to as Traumatic Brain Injury, TBI for short.
Over time, the damage to cerebral white matter is often associated with deficits in cognition, particularly in the attentional domain. For instance, a player with TBI might be more distracted by a fan in the stands and slower to react to the opposing team.
Based on previous work performed by Kraus and colleagues, this video demonstrates how to measure white matter integrity using DTI in patients with TBI compared to healthy control individuals.
We will also examine cognitive function using a selective attention task, explain how to analyze the imaging data, and interpret the relationship between diffusion values in defined regions of interest and attentional control.
In this experiment, two groups of participants—patients diagnosed with moderate to severe TBI and control individuals that are healthy—are scanned using a DTI protocol, and then tested on an attention task.
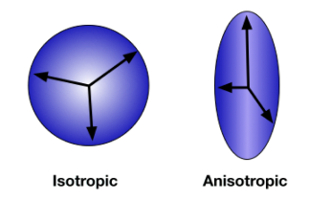
First, let’s discuss a few principles behind DTI: The technique is sensitive to the diffusion of water molecules, which are always moving, mostly in parallel to the vast amount of axonal bundles. This type of movement is known as anisotropic diffusion.
Along with the path of water flow, the amount of diffusion can be measured to compute the tensor—essentially illustrated as an ellipsoid with a direction. This value is quantified based on the relative length to its width using a method called fractional anisotropy, abbreviated as FA.
More specifically, FA values can range from 0—isotropic, or equal movement—to 1, which reflects the greatest amount of anisotropy.
The precision is maximized across all voxels by acquiring diffusion images during an MRI scan in many different directions that correspond to shifts in the applied magnetic field. This increased resolution occurs at the expense of time.
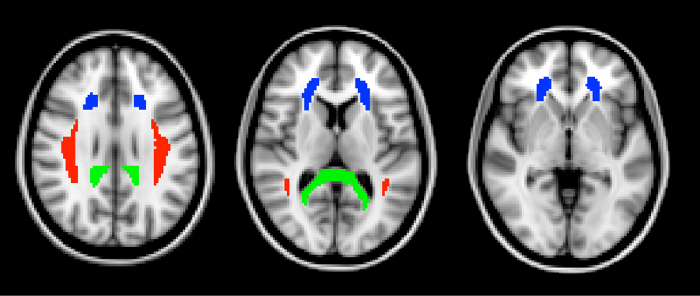
Knowing that, a critical dependent variable consists of the FA values for three regions of interest, or ROIs: the anterior corona radiata, the splenium of the corpus callosum, and the superior longitudinal fasciculus.
Compared to normal controls, the FA values are expected to be reduced in individuals with TBI, as their white matter is expected to be compromised in a non-localized manner, resulting in less anisotropy across all ROIs.
However, one region—the anterior corona radiata—is associated with connections to the anterior cingulate cortex, which plays an important role in attentional control.
To further explore this functional relationship between white matter integrity and behavior, all participants are tested on the Attention Network Task developed by Fan and colleagues.
In this paradigm, participants are asked to focus their attention, first towards a fixation cross that appears for a variable duration between 400 and 1600 ms, followed by two different types of arrows: a central one and two flanking groups that may vary in the direction they point.
In half of the trials, all of the arrows point in the same direction; these are considered to be congruent. For the other half, the center arrow points the opposite way of the flanking ones, and these cases are referred to as incongruent. Participants are asked to categorize the arrows by making associated keypresses as quickly as possible when each new set appears.
Here, the difference in reaction times between trial types is calculated as another dependent variable. Individuals who are more distracted by the flanking arrows are expected to have a larger difference score, which indicates poor attentional control.
This measure is therefore predicted to negatively correlate with the FA values, specifically in the region related to attentional ability—the anterior corona radiata—and not the others, thus showing functional significance of particular white matter tracts.
Prior to the experiment, recruit 20 adult patients that have been diagnosed with moderate to severe TBI within the last 6 months and age-matched controls, who have no history of neurological or psychological disorders.
For the purpose of this demonstration, test a patient that’s documented as having a loss of consciousness for more than 30 min or a score of < 13 on the Glasgow Coma Scale.
On the day of their scan, greet them and ensure that they do not suffer from claustrophobia or have any metal in their body; also have them fill out the necessary consent forms detailing the risks and benefits of the study.
After gaining consent, prepare the patient to enter into the scanning room. For more detailed information on the pre-scan procedures, please refer to another MRI project in this collection.
With the patient now in the scanner bore, first collect a high-resolution anatomical scan. Then, initiate a pulse sequence optimized for DTI by acquiring a B0 image—one that is not sensitive to diffusion direction—as well as multiple diffusion-weighted images in 64 different directions.
When the sequence is complete, escort the patient out of the scanner and into an experimental room with a computer to perform the next phase, an Attention Network Task.
Explain the task instructions: They will see a series of five arrows on the screen and should focus only on the center one. To ensure quick and accurate responses, have them place their hands on the keyboard, with their left index finger on the ‘F’ key and right one on ‘J’.
During trials where the center arrow is pointing left, instruct them to press ‘F’. Otherwise, when it is facing right, press ‘J’.
Allow the patient to complete 100 trials: Remember that each starts with a fixation cross that remains on the screen for a variable duration of 400 to 1600 ms, after which arrows appear, and the central one will either be incongruent or congruent.
Notice that the arrows remain on the screen until the patient responds, or for a maximum of 1700 ms if they don’t press either key. Also note that every trial ends with a fixation cross that remains visible for a total trial duration of 4 s.
At the end of the attention task, debrief the patient to conclude the study, and compensate them for their participation.
After the scanner and behavioral data have been obtained, the raw diffusion files first need to be converted into tensor images.
To begin preprocessing, perform distortion correction for eddy currents, which commonly occur in the raw data as a result of changing the magnetic field during acquisition.
To compensate for motion, apply a linear rigid-body affine transformation, which registers each of the directional diffusion images to the B0 reference.
In addition, isolate the brain from the skull and other non-neural tissues to ensure that tensors are not calculated for voxels outside of the brain.
Now, combine all 64 directional images to calculate the diffusion tensor at each voxel, and output the corresponding FA values in the background.
Subsequently, register the diffusion images to the high-resolution anatomical scan, and then to a standard atlas space to allow for group-level analysis.
With pre-processing completed, use a white matter atlas to identify three ROIs: the anterior corona radiata, the splenium of the corpus callosum, and the superior longitudinal fasciculus.
Finally, register each participant’s anatomical image to the standard atlas, and use these to warp the ROI masks into each participant’s brain space.
To graph the data, compare the extracted FA values by group, plotting each ROI separately. Notice that FA values were significantly lower in the TBI group in all three ROIs, indicating widespread white matter damage in those patients.
To incorporate the behavioral data, plot the differences in reaction times between incongruent and congruent trials against the FA values for all subjects. Perform a Pearson correlation analysis on these overall results, again independently for each ROI.
This time, only one of the regions—the anterior corona radiata—showed a significant correlation, in the negative direction. That is, high FA values were associated with fast reaction times, whereas low anisotropy corresponded to longer response times. These findings suggest a functional link between connecting white matter and attentional control.
Now that you are familiar with how to relate structure and function using DTI and an attentional control task, let’s look at how researchers are using similar approaches to study other populations with compromised connectivity or as a way to protect it.
While normal aging is associated with cognitive decline, changes aren’t necessarily widespread. Rather, they appear to be related to specific functions that correspond to white matter integrity and reduced FA values, especially in the prefrontal cortex. Thus, diffusion imaging could be used as a method for the early detection of age-related changes in executive function.
Using data collected by DTI, researchers can use a 3D technique called fiber tractography and reconstruct white matter tracts throughout the entire brain. This modeling procedure is useful across many domains, including neurosurgery.
If, for instance, surgeons need to remove a tumor, they can plan exactly where the white matter tracts are in proximity to critical structures and avoid detrimental consequences.
You’ve just watched JoVE’s introduction to diffusion tensor imaging. Now you should have a good understanding of how to design and conduct a DTI experiment, as well as how to analyze and interpret specific diffusion patterns with cognitive implications related to traumatic brain injury.
Thanks for watching!