While establishing a non-HA anastomosis rat OLT model using a previously described protocol28, our team observed 50% and 37.5% survival rates at 21 days and 60 days post-operation, respectively. Although high rates of long-term survival without HA anastomosis have been reported by some groups28, these early results highlight the drawbacks of not having arterial inflow. By contrast, the optimized HA reconnection procedure significantly increased long-term survival from 37.5% to 88.2% (p = 0.015) (Figure 6).
Histological analysis of a representative subset of transplanted animals without HA reconnection (at days 6 and 13 post-operation) showed signs of hypoxic liver injury with centrilobular necrosis (Figure 7). Extensive liver necrosis was associated with tremendously elevated levels of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) in these animals (Figure 7). In contrast, transplanted rats with HA reconnection showed no signs of liver injury, and histological analysis revealed a normal liver parenchyma structure with organized acini, lobules (e.g., central vein and portal triads with hepatic vein), arteries, and bile duct (Figure 7).
Although the mean anhepatic time over the course of 23 separate operations was acceptable (12 min and 14 s [± 78 s]), it is still possible that survival in the non-HA reconnection model can eventually be improved with increased practice. However, it is worth noting that three of the four animals transplanted without HA reconnection (which were being followed for long-term survival) were euthanized due to distress on days 56, 96, and 111 post-operation. Additionally, histological analysis of the livers revealed reactive changes after hypoxic liver injury including marked bile duct proliferation, periportal fibrosis and inflammation, and distorted liver parenchyma (Supplementary Figure 2). The presence of morphological features of hypoxic liver injury corroborate the findings that HA reconnection is important for efficient liver perfusion and normal function.

Figure 1: Schematic representation of the 3D-printed cuff design for portal vein and infrahepatic inferior vena cava. The first tie is tightened in the groove (ii) closest to the handle (iii), and the second tie is tightened in the groove (i) furthest away from the handle. The outside diameters are (iv) 2.38 mm for the portal vein (PV) and 2.15 mm for the infrahepatic inferior vena cava (IHVC). The inside diameters are (v) 1.74 mm for the PV and 1.38 mm for the IHVC. The lengths are (vi) 2.60 mm for the PV and 2.15 mm for the IHVC (exact specifications for all 3D-printed materials can be found in Supplementary Materials). Please click here to view a larger version of this figure.

Figure 2: Hepatic artery stent insertion in graft. (A) The opening end of the celiac trunk (i) is widened by cutting the splenic artery to the left gastric artery, which exposes the bifurcation of the common HA. (ii) The BD stent is tied prior to extraction of the donor rat liver. (iii) The PV cuff and (iv) IHVC cuff are inserted and tied by folding the ends of the vessels over the cuff. (B) (i) To insert the HA stent, the exposed common HA is stretched multiple times with forceps. (C) (i) The HA stent is placed securely in the common HA and tied with 8-0 prolene. (D) (i) The HA stent is flushed with (ii) Ringer's lactate solution (BD = bile duct, IHVC = infrahepatic inferior vena cava, HA = hepatic artery). Please click here to view a larger version of this figure.

Figure 3: Infrahepatic inferior vena cava connection using 3D-printed holder. (A) The (i) PV is connected using the same technique as the IHVC connection. The graft is (ii) clamped above the (iii) IHVC cuff. The recipient IHVC opening is (iv) sutured at the sides of the opening to a 3D-printed holder to keep it stretched open. A loose (v) 7-0 silk is tied around the recipient IHVC. (B) The cuff of the graft IHVC is (i) inserted within the recipient IHVC. The loose tie is now tightened. (C) The clamp is removed, and (i) the 3D printed holder is detached with scissors. (D) An additional (i) 7-0 silk is tied around the connection if not secure, but typically one tie is sufficient (PV = portal vein, IHVC = infrahepatic inferior vena cava). Please click here to view a larger version of this figure.

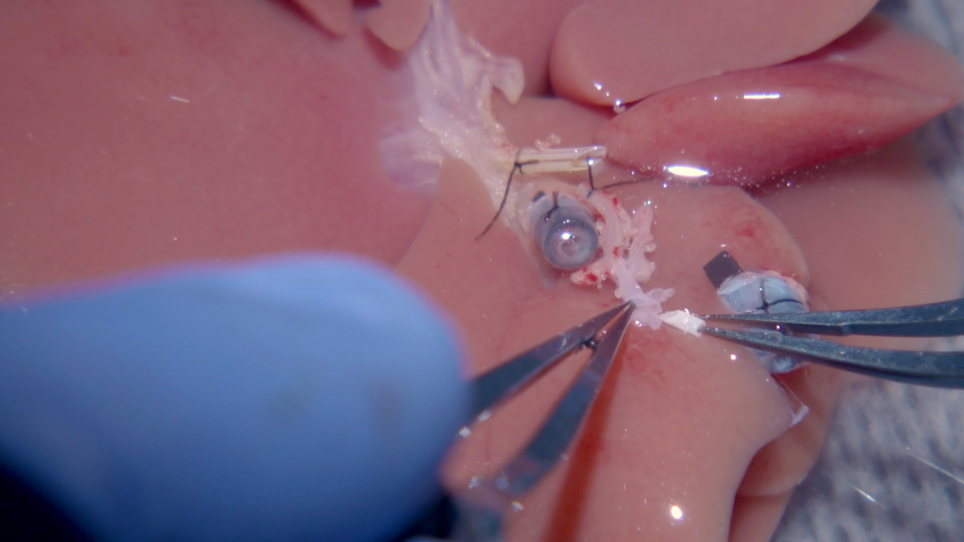
Figure 4: Microvascular sleeve connection of the hepatic artery. (A) (i) The BD stent is not connected to the recipient. (ii) The HA stent is placed in the graft, which is linked to the (iv) recipient's proper HA. (iii) The PV is connected. (B) 10-0 ethilon with a (i) curved needle is drawn through the HA stent to the sides of the recipient HA opening end. (C) The 10-0 ethilon is drawn back through the HA stent; therefore, the recipient's proper HA is pulled through the stent like a sleeve. (D) (i) A tie with 10-0 ethilon is made once the recipient's proper HA is pulled into the stent to the portion that first runs through the HA stent. (E) Shown here is a schematic of the HA anastomosis described in (B), (C), and (D) (BD = bile duct, HA = hepatic artery, PV = portal vein). *The opening end of the celiac trunk is widened by cutting the splenic artery to the left gastric artery. Please click here to view a larger version of this figure.

Figure 5: Bile duct connection using two stents. (A) (i) Graft BD stent is inserted into the recipient BD with the aid of the (ii) stent loosely tied at the opening of the recipient's BD. (iii) The PV is linked before the BD connection, which is located behind the BD. (B) The stent at the end of the recipient's BD is removed and used as a widened opening to (i) insert the BD stent tied to the graft. (C) The tie that is loosely securing the recipient stent is now used to tie the connection, and (i) another 7-0 silk is used to firmly keep the stent in place to avoid slipping or twisting of the stent. Please click here to view a larger version of this figure.

Figure 6: Transplant percent survival. Orthotopic rat liver transplantation without HA reconnection (n = 8) and with HA reconnection (n = 17). Animals are closely followed post-transplantation for signs of liver failure and/or infection for at least 60 days. Rats that showed no complications after surgery were considered survivors (*p = 0.015, as calculated by Kaplan-Meier estimation [long rank test]). Please click here to view a larger version of this figure.

Figure 7: Liver histopathological assessment. Representative hematoxylin and eosin-stained sections in animals (A) without and (B) with hepatic artery (HA) reconnection at days 6 and 13 after liver transplant (LTx). (C) Normal liver parenchyma showing portal triad (portal vein, artery, and bile duct), lobules including central vein, and acini. Hepatocytes next to the portal triad are zone 1 hepatocytes; hepatocytes next to the central vein within lobules are zone 3 hepatocytes; and hepatocytes between zones 1 and 3 are zone 2 hepatocytes (ALT = alanine aminotransferase, AST = aspartate aminotransferase, CV = central vein). Please click here to view a larger version of this figure.

Supplementary Figure 1: Stent and cuff dimensions. Please click here to view a larger version of this figure.

Supplementary Figure 2: Liver histopathological assessment showing disruption of liver parenchyma. Representative hematoxylin and eosin-stained sections in animals without HA reconnection at days 54, 96, and 111 after LTx. Please click here to view a larger version of this figure.
Supplementary Material 1: Porta cuff 200g – support 2.0. Please click here to view this file (Right click to download).
Supplementary Material 2: Cava cuff 200g – support 2.0. Please click here to view this file (Right click to download).
Supplementary Material 3: Liver retractor 200g. Please click here to view this file (Right click to download).
Supplementary Material 4: Back holder – 1.2. Please click here to view this file (Right click to download).
Supplementary Material 5: Cava 150g – 2.1. Please click here to view this file (Right click to download).
Supplementary Material 6: Porta 1.4.1. Please click here to view this file (Right click to download).
Supplementary Material 7: Holder arm McGil. Please click here to view this file (Right click to download).
Supplementary Material 8: Holder mini arm LAB. Please click here to view this file (Right click to download).
Supplementary Material 9: Holder and arm soft part 1.3. Please click here to view this file (Right click to download).
Supplementary Material 10: Holder base – 3.1. Please click here to view this file (Right click to download).