With this model, we induced severe TBI into adult, male, Wistar rats. Under the conditions we describe here, we typically observe mortality rates of 40-50%, and righting reflex times of 30 – 60 min as previously described20. We were able to collect video/EEG recordings 24 h/day beginning on the day of injury. A diagram showing the location of four monopolar EEG electrodes and a single reference electrode is shown in Figure 1A. Images which demonstrate the location and appearance of the TBI lesions expected with the conditions described here are shown in Figure 1B-D. Under the conditions described here, we consistently observe delta slowing within the first three days post TBI. Less severely injured rats exhibit unilateral, intermittent delta slowing (Figures 2C-D). In contrast, continuous, bilateral delta slowing is observed after more severe injuries (Figure 3C-D). Some degree of delta slowing was consistently observed in all TBI rats but was not detected in any sham operated (craniectomy only) control rats (Figures 2A-B; 3A-B). Extensive delta slowing was consistently observed during the first three days after injury in most TBI rats. Interestingly, rats typically show pronounced weight loss during the first three days post injury. Non-convulsive seizures are occasionally observed within the first week following TBI (Figure 4 C-D). Clinical seizures, presenting as spike clusters associated with rearing and falling as well as forearm clonus can be observed after 1-week post TBI (Figure 5C-D). Finally, Figure 6 presents representative images of occasional intermittent signal drop out and loss of signal due to battery failure.
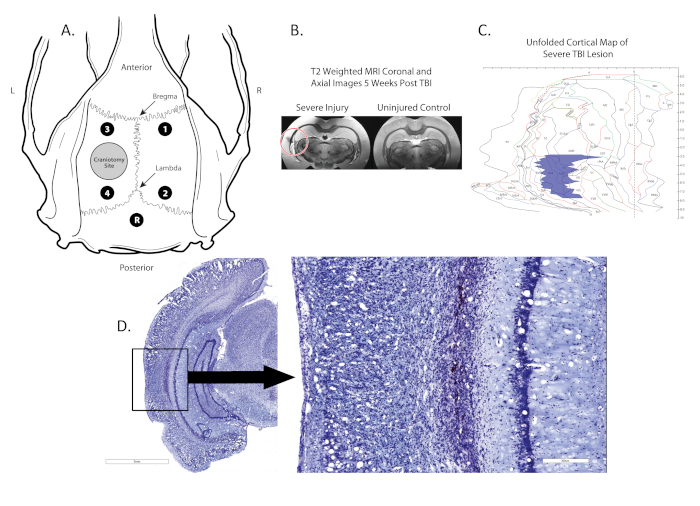
Figure 1. Location of craniectomy, electrode placement, and lesion. (A) shows a schematic diagram of the rat skull with the locations of the craniectomy (grey circle in the left hemisphere), four monopolar electrodes (Black dots; 1,2,3,4) located between the Bregma and Lambda and a reference electrode (Black dot, R) placed midline, posterior to the lambda; (B) shows coronal post-mortem T2 MRI scans with the location of the lesion identified by a red circle; (C) shows a 2-D map of the cortex where the location and size of the lesion is identified (blue region). (D) shows a Nissl stained coronal section with the lesion boxed, lesion is 100x magnified in image to the right. Please click here to view a larger version of this figure.
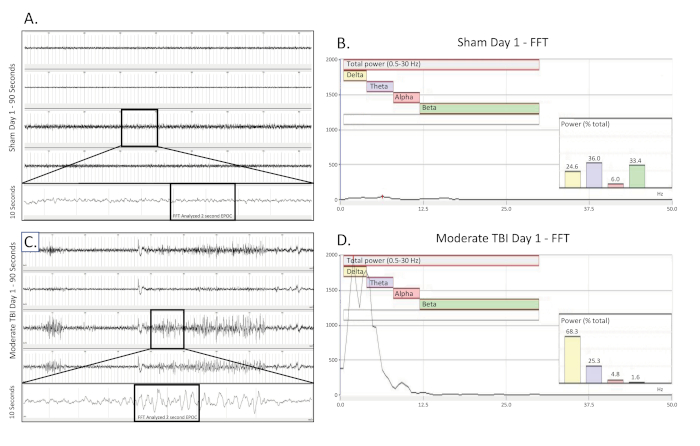
Figure 2. Unilateral, intermittent delta slowing collected on the day of a moderate TBI. (A) shows a 90 s EEG trace from a sham operated, uninjured control rat on the day of surgery. All four channels are presented. A 10 s long trace (taken from the boxed region) was extracted from the 3rd channel to better visualize the baseline EEG pattern. A 2048 ms EPOC section of this was then selected to be analyzed in the corresponding FFT. (B) FFT analysis of 2048 ms selected EPOC from the uninjured sham operated animal on the day of surgery. (C) shows a 90 s EEG trace, which demonstrates the intermittent, unilateral delta slowing pattern of a moderately injured animal on the day of injury. A 10 s long trace (taken from the boxed region) was extracted from the 3rd channel to better visualize the delta slowing EEG pattern. A 2048 ms EPOC section of this was then selected to be analyzed in the corresponding FFT. (D) FFT analysis of 2048 ms selected EPOC from the moderate TBI animal on the day of injury. 90 s EEG tracings, from top to bottom are biopotentials 1, 2, 3, 4, corresponding to their locations around the craniectomy site as seen in Figure 1. Grey vertical marks define 1 s intervals on the EEG traces. All EEG traces are shown on a scale of (±500 µV). Within FFT Analysis graphs, overall analyzed frequency range was 0.5-30 Hz. This was further broken down into 4 separate frequency bands of Delta (Yellow, 0.5-4 Hz), Theta (Purple, 4-8 Hz), Alpha (Red, 8-12 Hz), and Beta (Green, 12-30 Hz). % (Power) graph shown within the FFT analysis tells what percentage of the total power in the analyzed EPOC comes from each previously specified frequency band, allowing for further mathematical characterization of the EEG waveform patterns. Please click here to view a larger version of this figure.
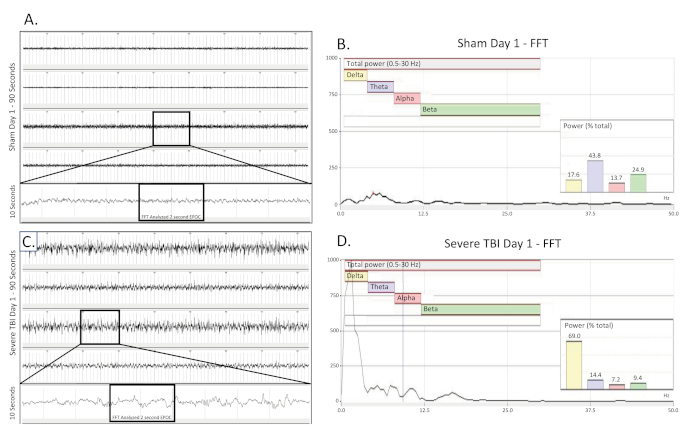
Figure 3. Bilateral, continuous delta slowing collected on the day of a severe TBI. (A) shows a 90 s EEG trace from a sham operated, uninjured control rat on the day of surgery. All four channels are presented. A 10 s long trace (taken from the boxed region) was extracted from the 3rd channel to better visualize the baseline EEG pattern. A 2048 ms EPOC section of this was then selected to be analyzed in the corresponding FFT. (B) FFT analysis of 2048 ms selected EPOC from the uninjured sham operated animal on the day of surgery. (C) shows a 90 s EEG trace, which demonstrates the continuous, bilateral delta slowing pattern of a severely injured animal on the day of injury. A 10 s long trace (taken from the boxed region) was extracted from the 3rd channel to better visualize the delta slowing EEG pattern. A 2048 ms EPOC section of this was then selected to be analyzed in the corresponding FFT. (D) FFT analysis of 2048 ms selected EPOC from the severe TBI animal on the day of injury. 90 s EEG tracings, from top to bottom are biopotentials 1, 2, 3, 4, corresponding to their locations around the craniectomy site as seen in Figure 1. Grey vertical marks define 1 s intervals on the EEG traces. All EEG traces are shown on a scale of (± 500 µV). Within FFT Analysis graphs, overall analyzed frequency range was 0.5-30 Hz. This was further broken down into 4 separate frequency bands of Delta (Yellow, 0.5-4 Hz), Theta (Purple, 4-8 Hz), Alpha (Red, 8-12 Hz), and Beta (Green, 12-30 Hz). % (Power) graph shown within the FFT analysis tells what percentage of the total power in the analyzed EPOC comes from each previously specified frequency band, allowing for further mathematical characterization of the EEG waveform patterns. Please click here to view a larger version of this figure.
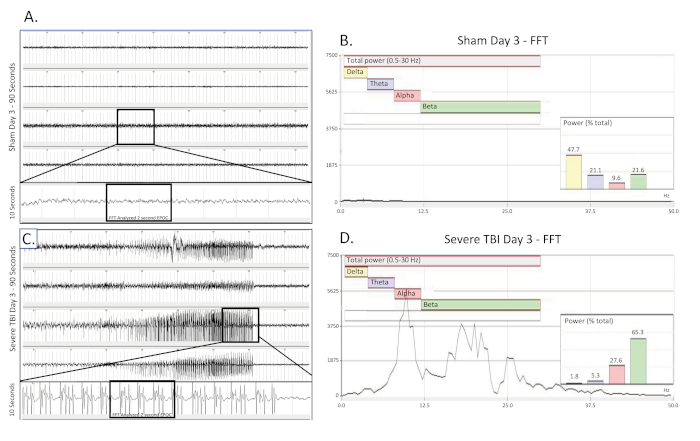
Figure 4. Nonconvulsive electrographic seizure collected 3 days post severe TBI. (A) shows a 90 s EEG trace from a sham operated, uninjured control rat 3 days25 after surgery. All four channels are presented. A 10 s long trace (taken from the boxed region) was extracted from the 3rd channel to better visualize the baseline EEG pattern. A 2048 ms EPOC section of this was then selected to be analyzed in the corresponding FFT. (B) FFT analysis of 2048 ms selected EPOC from the uninjured sham operated animal on the day three25 after of surgery. (C) shows a 90 s EEG trace three 25 days post severe injury. This show building, fast spiking pattern present bilaterally and across all 4 collecting channels. A 10 s long trace (taken from the boxed region) was extracted from the 3rd channel to better visualize the spiking EEG pattern. A 2048 ms EPOC section of this was then selected to be analyzed in the corresponding FFT. (D) FFT analysis of 2048 ms selected EPOC from the severe TBI animal on the day of injury. 90 s EEG tracings, from top to bottom are biopotentials 1, 2, 3, 4, corresponding to their locations around the craniectomy site as seen in Figure 1. Grey vertical marks define 1 s intervals on the EEG traces. All EEG traces are shown on a scale of (± 500 µV). Within FFT Analysis graphs, overall analyzed frequency range was 0.5-30 Hz. This was further broken down into 4 separate frequency bands of Delta (Yellow, 0.5-4 Hz), Theta (Purple, 4-8 Hz), Alpha (Red, 8-12 Hz), and Beta (Green, 12-30 Hz). % (Power) graph shown within the FFT analysis tells what percentage of the total power in the analyzed EPOC comes from each previously specified frequency band, allowing for further mathematical characterization of the EEG waveform patterns. Please click here to view a larger version of this figure.
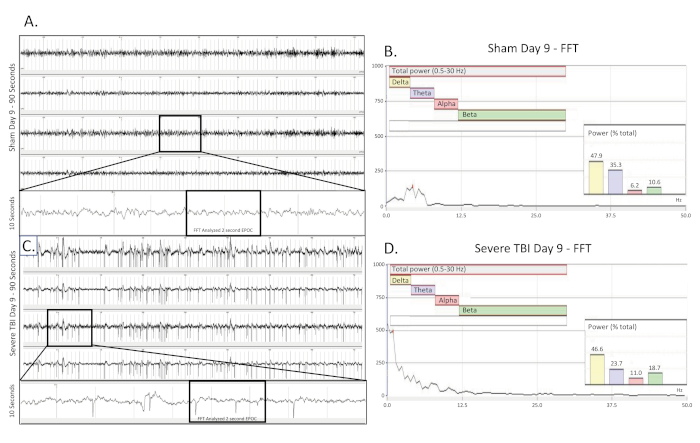
Figure 5. Convulsive electrographic seizure collected 9 days post TBI. (A) shows a 90 s EEG trace from a sham operated, uninjured control rat nine (9) days after surgery. All four channels are presented. A 10 s long trace (taken from the boxed region) was extracted from the 3rd channel to better visualize the baseline EEG pattern. A 2048 ms EPOC section of this was then selected to be analyzed in the corresponding FFT. (B) FFT analysis of 2048 ms selected EPOC from the uninjured sham operated animal on the day nine (9) after of surgery. (C) shows a 90 s EEG trace nine (9) days post severe injury. This show building, fast spiking pattern present bilaterally and across all 4 collecting channels. A 10 s long trace (taken from the boxed region) was extracted from the 3rd channel to better visualize the spiking EEG pattern. A 2048 ms EPOC section of this was then selected to be analyzed in the corresponding FFT. (D) FFT analysis of 2048 ms selected EPOC from the severe TBI animal nine (9) days post injury. 90 s EEG tracings, from top to bottom are biopotentials 1, 2, 3, 4, corresponding to their locations around the craniectomy site as seen in Figure 1. Grey vertical marks define 1 s intervals on the EEG traces. All EEG traces are shown on a scale of (± 500 µV). Within FFT Analysis graphs, overall analyzed frequency range was 0.5-30 Hz. This was further broken down into 4 separate frequency bands of Delta (Yellow, 0.5-4 Hz), Theta (Purple, 4-8 Hz), Alpha (Red, 8-12 Hz), and Beta (Green, 12-30 Hz). %(Power) graph shown within the FFT analysis tells what percentage of the total power in the analyzed EPOC comes from each previously specified frequency band, allowing for further mathematical characterization of the EEG waveform patterns. Please click here to view a larger version of this figure.
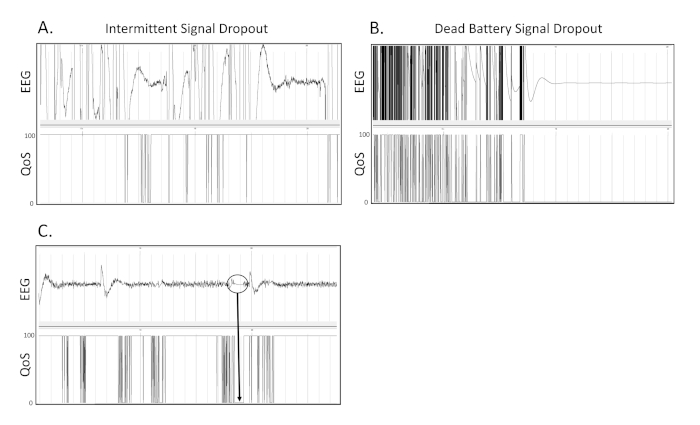
Figure 6. Signal drop out. These are 3 separate examples of what signal drop out due to transmitter or receiver issues appears as on the EEG recording. (A) This is an example of intermittent dropout of the EEG signal on a recording. (B) This is an example of drop out due to battery failure during continuous wireless telemetry appears as on an EEG tracing. (C) Within the circled region, it can be seen that when the Quality of Signal (QoS) drops from 100 to 0, the EEG tracing becomes flattened and stagnant at 0 µV. Grey vertical marks define 1 s intervals on the EEG traces. All EEG traces are shown on a scale of (± 500 µV). Please click here to view a larger version of this figure.
