All procedures were performed following the relevant guidelines and regulations and were approved by the Ethical Committee, WUM (KB/157/2017). Written consent was obtained from all participants, ensuring that they understood the general aim of the experiment and that they understood the inclusion of their data for statistical analysis purposes. All presented visual stimuli are generated using a Java-based desktop application (Viscacha2) created for the purpose of these experiments.
1. Setup
- Secure a quiet, dimmed room. Build a setup consisting of a computer, a keyboard, a flat display, an eye tracker (optional, depending on the research question and aims; see Table of Materials), a desk, a chinrest, and a chair. Arrange it so that the participants can sit with the chin resting on the chinrest, eyes directly in front of the center of the upper half of the display, and hands reaching the arrow keys on the keyboard. The horizontal distance between the display and the eyes should be 85 cm.
NOTE: Although the participants are trained and specifically asked to fixate the central fixation cross during the entire procedure, testing with an eye tracker may constitute an additional control for filtering during analyses of those participants who exhibit too many fluctuations with their gaze. Moreover, depending on the aim of the study, eye tracker results may provide interesting insight into the fixation patterns, pupil size, or location of interest of different cohorts of participants. - Visit https://github.com/grimwj/Viscacha2 and download the software by clicking the Code button and downloading ZIP. Extract the zip file and save it in the working directory.
- Follow the installation steps described in the README.txt file. In case of testing with an eye tracker, follow the software installation steps for the eye tracker. Mount the eye tracker as per instruction.
- To perform an initial check, run the program by double-clicking the Viscacha2.jar file. After the initial screen is displayed, press ESC on the keyboard to exit the program.
- Navigate through newly created folders – experiment_data, TestPatient, Shape_Brt. Open the .csv file using a spreadsheet editor (set semicolon as field separator). Verify that the parameters, such as screen dimensions and the distance from the screen, are correct.
NOTE: From here, the protocol is based on the assumption that a 1920 x 1080, 31.5 inch display is used and the distance between the patient and the screen is 85 cm. This implies that the screen occupies 44.6° of visual space horizontally. If these parameters cannot be met, one can refer to step 5 for reconfiguring the program.
2. Determining the initial difficulty of the test
- Open the config.txt file and find a line containing patient_name=TestPatient. Replace the TestPatient with a text identifying the subject being examined.
- In the config.txt file, find the line filename=Shape_Brt.txt. Make sure that this line does not begin with a hash symbol # (uncommented line).
- Ask the subject to sit in front of the display, with his/her chin rested and eyes directly in front of the center of the upper half of the display. Verify that the distance from the screen is correct. Make sure that the keyboard keys are easily accessible for the subject to use.
- Navigate to the Viscacha2.jar directory and run the program. Teach the participant to focus the sight on the fixation cross at the center of the screen for the entire duration of the experiment.
- On each side of the screen, either a circle or an ellipse will be presented at the same distance from the central fixation cross. The task is to select the circle over an ellipse using the left and right arrow keys on the keyboard. Explain the task to the participant, and when he/she is ready, press the s key to begin the experiment. The experiment continues till the participant presses one of the arrow keys.
- The program ends after four reversals have occurred or a maximum number of trials has been reached. A reversal occurs when the subject selects the wrong response after previously selecting the correct one or vice versa.
NOTE: This is a staircase-type procedure. The difficulty of each trial increases after each correct response and decreases after a wrong response. Figure 1 displays how the staircase level changes over trials for one representative participant. - Note the four reversals after which the task is finished and the detection threshold has been established. Open the corresponding .csv file containing results. Locate the THRESHOLD columns near the end of the file. Use the value in this column to calculate the initial difficulty for subsequent tasks.
NOTE: The test can also be presented in a constant paradigm, where the level of the difficulty is fixed and does not change, by removing the hash symbol from the Experiment_Type=Constant line in the init.txt files and by adding a hash symbol before the line Experiment_Type=Staircase.

Figure 1: Change in the staircase level over the duration of the Shape_Brt experiment (subsequent trials). The red plot depicts the staircase level, which translates to the aspect ratio of the S- (ellipse). After 4 reversals have occurred (blue bars), the subject’s detection threshold has been established, and the task is finished. Please click here to view a larger version of this figure.
- Use the newly obtained threshold as the baseline for the next stimuli presentation (steps 2.3–2.5). To replace the new threshold in all the stimuli definition files, use the Python script inside the replacer folder and follow the instructions on the screen.
3. Stimuli procedure
NOTE: A total of 10 experiments will be conducted: 5 with white dots on a black background and 5 with black dots on a white background.
- Coherence task
- When the subject is ready, open the config.txt file and comment (i.e., insert the hash symbol) the line filename=Shape_Brt.txt and uncomment the line below, including the shape_dotsB_C.txt task. In this task, the circle and the ellipse consist of dots moving randomly with a velocity of 10°/s. The background is built of dots moving coherently upward with the same velocity as in the circle and ellipse.
NOTE: It is possible to define a different movement direction of the background dots by editing the Direction parameter inside the definition file for each task. - Run Viscacha2.jar. Explain the task to the subject in simple words, for example, Please always point to the circle. When the participant is ready, press the s key to begin the experiment. Wait until the experiment is completed.
- Open the config.txt file, comment the line filename=shape_dotsB_C.txt, and uncomment the line below including the shape_dotsW_C.txt task. Repeat step 3.1.2.
- When the subject is ready, open the config.txt file and comment (i.e., insert the hash symbol) the line filename=Shape_Brt.txt and uncomment the line below, including the shape_dotsB_C.txt task. In this task, the circle and the ellipse consist of dots moving randomly with a velocity of 10°/s. The background is built of dots moving coherently upward with the same velocity as in the circle and ellipse.
- Direction task
- When the subject is ready, open the config.txt file and comment on the previously selected filename. Uncomment the line containing filename=shape_dotsB_D.txt task. In this task, the circle and the ellipse consist of dots moving coherently upward with a velocity of 10°/s. The background consists of dots moving coherently leftward with the same velocity as in the circle and ellipse.
- Run Viscacha2.jar. Explain the task to the subject. When the participant is ready, press the s key to begin the experiment. Wait until the experiment is completed.
- Open the config.txt file, comment the line filename=shape_dotsB_D.txt, and uncomment the line below, including the shape_dotsW_D.txt task. Repeat step 3.2.2.
- Velocity task
- When the subject is ready, open the config.txt file and comment the previously selected filename. Uncomment the line containing filename=shape_dotsB_V10_20.txt task. This task involves three conditions. The circle and ellipse and the background consist of dots moving coherently upward, and dots within the circle and the ellipse always move slower than the background dots: i) 10°/s versus 20°/s; ii) 5°/s versus 10°/s; and iii) 1°/s versus 2°/s.
- Run Viscacha2.jar. Explain the task to the subject. When the participant is ready, press the s key to begin the experiment. Wait until the experiment is completed.
- Open the config.txt file and comment on the line shape_dotsB_V10_20.txt and uncomment the line below, including the shape_dotsW_V10_20.txt task. Repeat step 3.2.2.
- Repeat steps 3.3.1 – 3.3.3 2x, for tasks shape_dotsB_V5_10.txt and shape_dotsW_V5_10.txt, as well as for shape_dotsB_V1_2.txt and shape_dotsW_V1_2.txt.
- To avoid manually changing the filename for each task after the task is done, use a sweep_file option. In the config.txt file, set the sweep_files field to 0 to end the procedure after each task procedure is over.
- Use this setting for the Shape_Brt.txt task to define the initial baseline threshold value. Once the baseline is set, for running multiple tasks in succession, set the sweep file to an integer between 1 and 9. The integer here determines the number of changes between consecutive tasks (e.g., if set to 1 and shape_dotsB_D.txt is uncommented, the program will run this task and the next one. If set to 9, all tasks will be run). Internally, this will result in regenerating a new config file after each experiment is completed, with a previously selected filename commented and the subsequent filename selected for the upcoming experiment.
4. Goggles limiting vision
- To transiently remove the peripheral visual field, use swimming goggles (Figure 2), where transparent lenses are replaced with white opaque ones. The lenses had an aperture of 1.4 mm that limited the visual field to the central 10°. To make the goggles suitable for every subject and to account as best as possible for the natural individual interocular distance, make 14 pairs of goggles with holes spacing from 58 mm to 72 mm (with a step of 1 mm between each pair of goggles).

Figure 2: Narrowing goggles. The central holes have a diameter of 1.4 mm. We had 14 pairs of goggles with distances between holes of 58 mm to 72 mm. Please click here to view a larger version of this figure.
- Use a ruler to define the distance between the participant’s eyes. Place the ruler just above the eyes, in line with the eyebrows, with the value 0 on top of one eye. Calculate how far in mm, is the second pupil by checking the value on top of the second eye. During the procedure, ask the participant to maintain the gaze as stable as possible.
- After the more suitable pair has been chosen, give a break of 15 min. During this time, ask the participants to move freely in the room, use their telephone, or read to let the eyes become accustomed to the new visual condition.
- Start the procedure again from step 3.
5. Reconfiguration
- Screen size and distance calibration
- If a different display is being used, insert the screen dimensions (resolution and diagonal) into the config file (resolution_v for vertical resolution, resolution_h for horizontal resolution, diagonal_inch for the screen diagonal in inches).
- Run Viscacha2.jar. Once the initial screen displays, press ESC to terminate. Open the .csv file containing the results.
- Find the line containing Distance mm text and write down the value.
- Readjust the experimental setup so that the subject can be seated at the newly calculated distance. Calculate the distance so that the screen width occupies 44.6° of visual space horizontally. This is defined by the full_angle_h parameter, which can also be changed in the config.txt file.
NOTE: Calibration can be also performed for screen height using the full_angle_v parameter. Please note that only one of these parameters can be set, the other one has to be commented with a # prefix.
- Stimuli definition
- Define the stimuli parameters in separate files (e.g., shape_dotsB_C.txt). Some values, such as dimensions of the S- (Ellipse_X, Ellipse_Y) are given in pixels. To calculate from pixels to visual degrees, multiply the value by the Pixel to angle multiplier extracted from the csv file containing results.
NOTE: Stimuli parameters, such as the coherence of the dots are predefined and adjustable for each layer (background, shape S+, shape S-, noise). In the coherence task, for example, the circle and the ellipse consist of dots moving randomly with a velocity of 10°/s (coherence = 0.0). The background is built of dots moving coherently upward with the same velocity as in the circle and ellipse (coherence = 1.0). Viscacha2 does not have an official user manual as of yet. For further information regarding the stimuli definition refer to the stimuli_description.ods file in the Viscacha2 repository.
- Define the stimuli parameters in separate files (e.g., shape_dotsB_C.txt). Some values, such as dimensions of the S- (Ellipse_X, Ellipse_Y) are given in pixels. To calculate from pixels to visual degrees, multiply the value by the Pixel to angle multiplier extracted from the csv file containing results.
The motion acuity task generates, for each participant, one result file for each stimuli procedure. An exemplary log file for a test participant has been included in the repository inside the doc folder. From row 1 to row 31, various settings are reported, such as the name of the patient and the configuration settings. The task block starts from row 34 and reports important information necessary for further analysis: event time, event type, trial, duration, selection, correct, success, experimenter, external stimuli, reversal, and staircase level. Importantly, selection and success columns should not be empty; in this case, it may indicate a malfunctioning of the response tool (keyboard or response pad). From line 170, the threshold value is reported under the column threshold. Note that the linked repository in step 1.2 includes a log file preparation script for cleaning the log files. The log file can be used for analyzing the accuracy of the responses by comparing the column's selection and correcting or by simply checking the column named success. Another useful value reported is the duration time for reaction time investigation.
For a study about the motion-acuity threshold instead, the crucial variable is the value below the column threshold. Each participant will have one threshold for each stimulus presentation, and it is possible to compare thresholds deriving from different contrasts and/or from different tasks.
In Figure 3, a representative plot for a control group that has been tested in full vision condition (i.e., without wearing narrowing goggles; Figure 3A,B) and in limited vision condition (wearing narrowing goggles; Figure 3C,D) is shown. The included control participants had normal or corrected-to-normal vision.

Figure 3: Representative results for the control group. (A, B) Results for testing in full vision and (C,D) in limited vision with goggles covering the peripheral visual field. The motion-acuity thresholds from fast velocity (10/20 deg) to coherence tasks are shown in (A, C) negative left panels and (B, D) positive contrast in right panels. On the vertical axis, the motion-acuity threshold is reported as the minimal perceived difference in visual degrees. The individual thresholds are shown as a circle. Means and standard errors are shown. Please click here to view a larger version of this figure.
In Figure 4, two groups of patients were tested: patients suffering from peripheral photoreceptor degeneration (Retinitis pigmentosa, RP; Figure 4A,B) and patients suffering from central photoreceptor degeneration (Stargardt, STGD; Figure 4C,D). To correctly include patients, the final diagnosis was established after typical ophthalmological examination and after accessory investigations, such as optical coherence tomography (OCT), fluorescein angiography (FA), and electrophysiological testing (flash electroretinography, FERG). Furthermore, if patients were not able to see or perform the baseline task (Shape_Brt.txt) for determining the initial difficulty of the test, they were automatically excluded from the procedure.
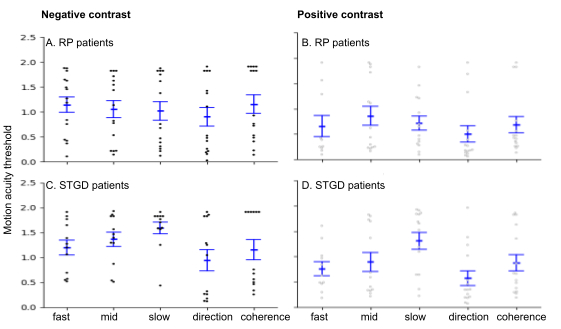
Figure 4: Representative results for RP and STGD patients. (A, B) Results for RP patients with loss of visual periphery and (C, D) STGD patients with loss of central vision. The motion-acuity thresholds from fast velocity (10/20 deg) to coherence tasks are shown in (A, C) negative left panels and (B, D) positive contrast in right panels. On the vertical axis, the motion-acuity threshold is reported as the minimal perceived difference in visual degrees. The individual thresholds are shown as a circle. Means and standard errors are shown. Please click here to view a larger version of this figure.
In Figure 3 and Figure 4, on the vertical axis, the acuity threshold is reported as the minimal perceived difference; the horizontal axis divides the results into tasks: fast 10/20, mid 5/10, and slow 1/2, in fast velocity direction and coherence. Tasks are presented in two contrasts (i.e., a and c for negative, b and d for positive). Each participant is reported as a single point, while error bars represent the standard error.
These representative results show that for the control group in full vision (Figure 3A), the motion-acuity threshold is similar among the tasks. With the most demanding task velocity 10/20 in negative contrast, the easiest slow velocity 1/2 in positive contrast. Note that wearing the goggles covering the peripheral visual field, as shown in the limited visual condition, reduced the spread of results among participants, revealing a successful measurement of central and peripheral visual stimulation (Figure 3B). For the patients (Figure 4), it is also shown with the velocity tasks how the visual impairment affects the motion-acuity threshold. For RP patients (Figure 4A,B), who have spared the central visual field, the slowest tasks are the easiest, while for the STGD patients (Figure 4C,D) who have spared peripheral visual field, the pattern follows the opposite trend showing higher threshold for the velocity 1/2 (slow) and lower threshold for the velocity 10/20 (fast). In contrast, the direction and coherence tasks did not differentiate the two patient groups.
Representative films of the stimuli are available in .mp4 format in Supplementary File 1, Supplementary File 2, Supplementary File 3, Supplementary File 4, Supplementary File 5, Supplementary File 6, Supplementary File 7, Supplementary File 8, Supplementary File 9, Supplementary File 10, Supplementary File 11. Please note in those recordings, the white cursor shows the position of the circle (stimulus S+), which is to be chosen for a correct choice. During the experimental session, this cursor is not visible. The recordings are available for the baseline task Shape_Brt, the coherence tasks (shape_dotsB_C and shape_dotsW_C), the direction tasks (shape_dotsB_D and shape_dotsW_D) and the velocity tasks (fast 10/20 deg: shape_dotsB_V10_20, shape_dotsW_V10_20; mid 5/10 deg: shape_dotsB_V5_10, shape_dotsW_V5_10; slow 1/2 deg: shape_dotsB_V1_2, shape_dotsW_V1_2), in negative and positive contrasts.
Supplementary File 1: Baseline task for calculating the initial threshold. The circle and ellipse are shown on the side of the fixation cross. After each choice, the ellipse changes its shape: in case of correct response (the participant chooses the circle), the shape of the ellipse becomes more similar to a circumference; in case of wrong response (the participant chooses the ellipse), the shape of the ellipse becomes more accentuate, following the staircase procedure. Throughout the entire procedure, the participant is asked to look at the fixation cross. Please click here to download this file.
Supplementary File 2: Coherence task in negative contrast. The RDK is built with black dots moving on a white background. The two centrally located shapes are defined by the RDK motion: inside the shapes, the dots move randomly, while the background is formed with dots moving upwards at 10°/s. The level of difficulty is set with the baseline task. The circle and ellipse are shown on the side of the fixation cross. Throughout the entire procedure, the participant is asked to look at the fixation cross. Please click here to download this file.
Supplementary File 3: Coherence task in positive contrast. The RDK is built with white dots on a black background. The two centrally located shapes are defined by the RDK motion: inside the shapes, the dots move randomly, while the background is formed with dots moving upwards at 10°/s. The level of difficulty is set with the baseline task. The circle and ellipse are shown on the side of the fixation cross. Throughout the entire procedure, the participant is asked to look at the fixation cross. Please click here to download this file.
Supplementary File 4: Direction task in negative contrast. The RDK is built with black dots moving on a white background. The two centrally located shapes are defined by the RDK motion: inside the shapes, the dots move upwards at 10°/s, and the background moves leftward at 10°/s. The initial level of difficulty is set as in Supplementary File 2. The circle and ellipse are shown on the side of the fixation cross. Throughout the entire procedure, the participant is asked to look at the fixation cross. Please click here to download this file.
Supplementary File 5: Direction task in positive contrast. The RDK is built with white dots moving on a black background. The two centrally located shapes are defined by the RDK motion: inside the shapes, the dots move upwards at 10°/s, and the background moves leftward at 10°/s. The initial level of difficulty is set as in Supplementary File 2. The circle and ellipse are shown on the side of the fixation cross. Throughout the entire procedure, the participant is asked to look at the fixation cross. Please click here to download this file.
Supplementary File 6: Fast velocity task in negative contrast. The RDK is built with black dots moving on a white background. The two centrally located shapes are defined by the RDK motion: inside the shapes, the dots move upwards at 10°/s, and the background moves upwards at 20°/s. The initial level of difficulty is set as in Supplementary File 2. The circle and ellipse are shown on the side of the fixation cross. Throughout the entire procedure, the participant is asked to look at the fixation cross. Please click here to download this file.
Supplementary File 7: Fast velocity task on positive contrast. The RDK is built with white dots moving on a black background. The two centrally located shapes are defined by the RDK motion: inside the shapes, the dots move upwards at 10°/s, and the background moves upwards at 20°/s. The initial level of difficulty is set as in Supplementary File 2. The circle and ellipse are shown on the side of the fixation cross. Throughout the entire procedure, the participant is asked to look at the fixation cross. Please click here to download this file.
Supplementary File 8: Mid-velocity task in negative contrast. The RDK is built with black dots moving on a white background. The two centrally located shapes are defined by the RDK motion: inside the shapes, the dots move upwards at 5°/s, and the background moves upwards at 10°/s. The initial level of difficulty is set as in Supplementary File 2. The circle and ellipse are shown on the side of the fixation cross. Throughout the entire procedure, the participant is asked to look at the fixation cross. Please click here to download this file.
Supplementary File 9: Mid-velocity task in positive contrast. The RDK is built with white dots moving on a black background. The two centrally located shapes are defined by the RDK motion: inside the shapes, the dots move upwards at 5°/s, and the background moves upwards at 10°/s. The initial level of difficulty is set as in Supplementary File 2. The circle and ellipse are shown on the side of the fixation cross. Throughout the entire procedure, the participant is asked to look at the fixation cross. Please click here to download this file.
Supplementary File 10: Slow velocity task in negative contrast. The RDK is built with black dots moving on a white background. The two centrally located shapes are defined by the RDK motion: inside the shapes, the dots move upwards at 1°/s, and the background moves upwards at 2°/s. The initial level of difficulty is set as in Supplementary File 2. The circle and ellipse are shown on the side of the fixation cross. Throughout the entire procedure, the participant is asked to look at the fixation cross. Please click here to download this file.
Supplementary File 11: Slow velocity task in positive contrast. The RDK is built with white dots moving on a black background. The two centrally located shapes are defined by the RDK motion: inside the shapes, the dots move upwards at 1°/s, and the background moves upwards at 2°/s. The initial level of difficulty is set as in Supplementary File 2. The circle and ellipse are shown on the side of the fixation cross. Throughout the entire procedure, the participant is asked to look at the fixation cross. Please click here to download this file.
