The absolute indicator of success following use of the SEEG methodology is seizure freedom for the patient, which ultimately follows successful electrode implantations, successful electrophysiological recordings, as well as successful resection of the EZ. Such a case is shown in Figure 1. Panels A and B of Figure 1 show two tests (single positron emission computed tomography (SPECT) and magnetoelectroencephalography (MEG), respectively) that help in the creation of the AEC hypothesis. However, discussion of the identification of the EZ and the completion of the subsequent resection is outside the scope of this article. However, when SEEG evaluation demonstrates that a patient is a poor surgical candidate for any number of reasons (AEC overlaps with eloquent cortex, multifocal epiliptogenicity, etc.) helping a patient to avoid surgery may certainly be classified as a successful study. Here the focus is instead on the successful anatomical placement of the electrodes and the absence of complications as the indicator for success using this methodology. As such, Figure 1C demonstrates the positioning of an electrode in the frontal opercular and dorsal insular area. Figure 1D shows the resection of the right operculum and insula in a post-operative T1 MRI image.
Figure 2 demonstrates the appropriate OR setup, successful bolt placement, and successful electrode implantation for the SEEG methodology. In a study of 200 patients who underwent a total of 2,663 SEEG electrode implantations at our center only 5 patients experienced complications. The rates of wound infection, hemorrhagic complications, and transient neurological deficit were 0.08%/electrode, 0.08%/electrode, and 0.04%/electrode for a total morbidity rate of 2.5%/patient and a mortality rate of 0%/patient.
| Clinical Scenario | Method of Choice | Second Option |
| Lesional MRI: Potential epileptogenic lesion is superficially located, near or in the proximity of eloquent cortex. -OR- Non-lesional MRI: Hypothetical EZ located in proximity of eloquent cortex |
SBG | SEEG |
| Lesional MRI: Potential epileptogenic lesion is located in deep cortical and subcortical areas. -OR- Non-lesional MRI: Hypothetical EZ is deeply located or located in non-eloquent areas. |
SEEG | SBG with depths |
| Need for bilateral explorations and/or reoperations | SEEG | SBG with depths |
| After subdural grids failure | SEEG | SBG with depths |
| When the AEC hypothesis suggests the involvement of a more extensive multilobar epileptic network. | SEEG | SBG with depths |
| Suspected frontal lobe epilepsy in non-lesional MRI scenario. | SEEG | SEEG |
Table 1. Selection criteria for SDG (with or without depth electrodes) vs. SEEG for invasive monitoring of patients with medically refractory focal epilepsy.
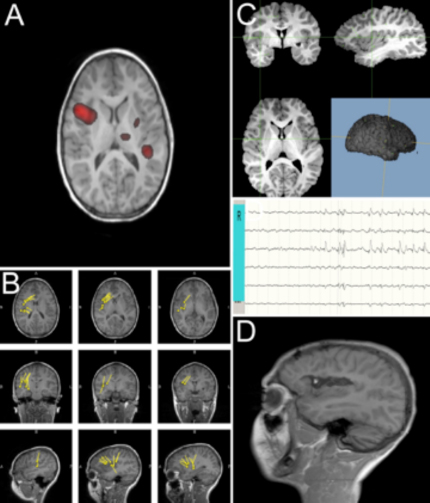
Figure 1: Components of the STEREO-ELECTRO-ENCEPHALOGRAPHY methodology. Panels A and B are showing non-invasive pre-implantation localization testings (as ictal SPECT – A, and MEG scan – B) demonstrating potential epileptogenicity located in the right opercular-insular areas. Panel C depicts the location of the R electrode, in the frontal opercular and dorsal insular area, from which epileptic activity was demonstrated by local field potentials. Panel D depicts post-operative T1 MRI image (sagittal view), demonstrating right opercular and insula resection. Please click here to view a larger version of this figure.

Figure 2: STEREO-ELECTRO-ENCEPHALOGRAPHY robotic method. The figure represents an intra-operative digital picture of the robotic technique, during the drilling phase. The robotic arm precisely guides the drilling step, allowing (after opening the dura and the position of the guiding bolt) the final implantation of the depth electrode. The robotic arm is equipped with a 2.55 mm adapter, which allows precise alignment of the 2.5 mm drill bit. Please click here to view a larger version of this figure.
