For ECochG measurements during cochlear implantation, a standardized procedure is important to achieve the highest possible reproducibility of signals. Here, a setup is proposed wherein the surgeon and the engineer sit opposite each other to facilitate communication (Figure 1). When setting up the system, it is important that there is an unimpeded stimulus transmission. For example, the ear canal should be completely cleaned and clear; the eartip must sit deep in the ear canal; the eartip and sound tube are not kinked; the sound tube must run visibly on the sterile cover and be accessible during surgery; the retractor does not impact the ear canal, and thorough hemostasis should be done prior to the insertion process to ensure an air-filled middle ear space. In addition, a stable connection between the transmitting and receiving coils is important to prevent interruptions during the insertion process. Therefore, the sterile drapes should be as thin as possible (Figure 2), the skin thickness must be checked at the beginning of the surgery, and the two magnets should be aligned. Furthermore, when starting the ECochG measurement, the implant housing must be covered by soft tissue, and the impedance should be checked before continuing with the insertion.
Using this measurement protocol, we performed measurements with 12 patients (Table 2). These patients had a maximum hearing threshold of 100 dB HL at 500 Hz. When calculating the PTA, the mean of the hearing thresholds was taken at 125 Hz, 250 Hz, and 500 Hz. ECochG recordings were performed using an acoustic stimulus at 500 Hz, condensation polarity, and 30 dB above the individual hearing threshold (minimum 100 dB HL, maximum 120 dB HL). The acoustic stimulus had a duration of 8 ms, with a rise/fall time of 2 ms each22. In total, 100 recordings were taken in each case. For signal processing, the focus was on cochlear microphonic signals using Python. First, we applied bandpass filtering (Butterworth, 4th order, 100 Hz-3 kHz bandpass) in forward-backward mode. Finally, an ECochG response was considered valid if the signal-to-noise ratio (SNR) was greater than one. SNR was calculated using the ± averaging method23. The SNR estimate fluctuates due to the small number of epochs. Therefore, the SNR calculation is repeated 1000 times with random subdivisions to obtain a robust estimate. Example measurements are shown in Figure 3: the ECochG signal amplitude increases with its maximum at electrode 9. The mid-peak pattern can be confirmed in the postinsertion measurements (fully inserted electrode). Considering these results, the mid-peak pattern was measured in 8 out of 12 subjects. Others showed an apical-peak (subjects 1, 4, 6) or a start-peak (subject 3)
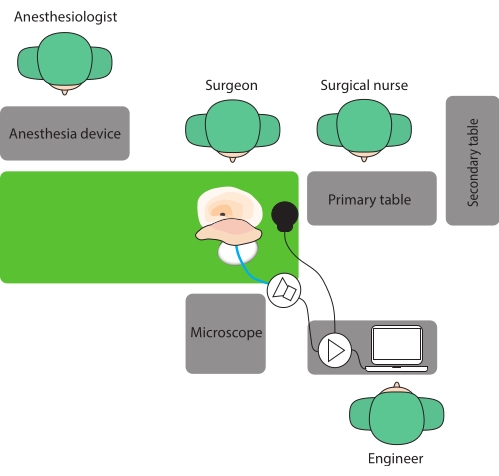
Figure 1: Operative room setup. Here, a setup is proposed where the surgeon and the engineer sit opposite each other to facilitate communication. Please click here to view a larger version of this figure.

Figure 2: Draping before the surgery. Care must be taken to ensure that there is a stable connection between the transmitting and receiving coils. (A) Thin, sterile drapes and (B) the fluid bag positioned as low as possible shorten the distance between the two coils. In this way, a good connection to the implant can be achieved. (C) The eartip must sit deep in the ear canal. (D) Using a large swab avoids strong buckling of the eartip and sound tube as well as eartip displacement. Please click here to view a larger version of this figure.
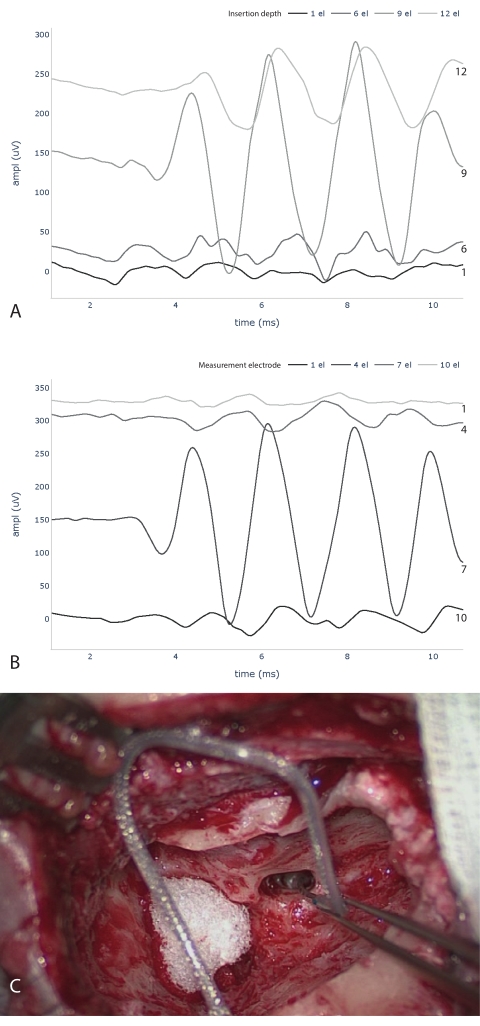
Figure 3: Intraoperative ECochG measurements. ECochG traces during (A) and after (B) electrode insertion are shown. Please note that the numbering of electrodes for A and B starts at opposite ends. (A) measures at the electrode tip and counts the number of electrodes inserted into the cochlea. (B) indicates the measurement electrodes, starting with the tip electrode as number one. Below (C), image taken during the implantation process with six inserted electrodes. Abbreviations: ECochG = electrocochleography; ampl = amplitude; el = electrode. Please click here to view a larger version of this figure.
| AB | Cochlear | Med-El | |
| Computer | Tablet AIM | Arbitrary | Arbitrary |
| Software | OMSuite | Cochlear Research Platform | Maestro |
| Implant interface | Audio processor, coil cable | Audio processor, coil cable | Coil cable |
| Interface connection | Programming cable | Cochlear Programming Pod, programming cable, USB | MAXInterface, USB |
| Acoustic stimulation | Transducer AIM | Transducer Cochlear | Arbitrary waveform generator, Transducer Etymotic, trigger cable |
| Sound tube | Custom | Etymotic | Etymotic |
| Eartip | Custom | Etymotic | Etymotic |
Table 1: Hardware and software required for ECochG recordings by three different manufacturers. Abbreviation: ECochG = electrocochleography.
| Subject | Electrode (inserted ec) | Cochlear access | Pre PT at 500 Hz (dB HL) | Pre PTA (dB HL) | Post PT at 500 Hz (dB HL) | Post PTA (dB HL) | IOS SNR | IEC | Final SNR |
| 0 | Flex 28 (11) | rw | 100 | 80 | 115 | 101.7 | 8.68 | 10 | 2.32 |
| 1 | Flex 28 (12) | rw | 65 | 46.7 | 85 | 68.3 | 1.22 | 12 | 1.22 |
| 2 | Flex 28 (12) | rw | 65 | 56.7 | 110 | 98.3 | 2.27 | 9 | 0.77 |
| 3 | Flex 28 (12) | rw | 100 | 91.7 | 110 | 106.7 | 1.35 | 1 | 0.95 |
| 4 | Flex 28 (12) | rw | 100 | 100 | 125 | 111.7 | 1.78 | 12 | 1.78 |
| 5 | Flex 24 (11) | c | 70 | 58.3 | 125 | 111.7 | 3.42 | 9 | 0.91 |
| 6 | Flex 28 (12) | rw | 80 | 45 | 110 | 91.7 | 22.9 | 12 | 22.9 |
| 7 | Flex 28 (12) | rw | 55 | 53.3 | 125 | 111.7 | 2.9 | 6 | 1.43 |
| 8 | Flex 28 (12) | rw | 70 | 70 | 105 | 80 | 2.87 | 6 | 1.44 |
| 9 | Flex 28 (12) | rw | 55 | 40 | 105 | 68.3 | 37.8 | 9 | 5.3 |
| 10 | Flex 28 (11) | rw | 65 | 58.3 | 100 | 90 | 29.14 | 9 | 13.5 |
| 11 | Flex 28 (12) | rw | 80 | 78.3 | 100 | 85 | 3.83 | 6 | 1.89 |
Table 2: ECochG recordings during CI surgery in 12 subjects. ECochG recordings during CI surgery in 12 subjects. IOS SNR displays the maximum SNR of the cochlear microphonic signal reached during insertion. IEC shows at how many inserted electrodes this maximum SNR was reached. The final SNR shows the CM amplitude of the fully inserted electrode at the most apical position. Abbreviations: ECochG = electrocochleography; CI = cochlear implant; rw = round window; C = cochleostomy; IEC = inserted electrode contacts; IOS = intraoperative signal; apical = most apical electrode; pre = preoperative; post = postoperative (4 weeks); PT = pure tone threshold; PTA = pure tone average; SNR = signal-to-noise ratio.
