Successful procedure, transduction and transcription
Figure 1 shows the parotid papilla adjacent to the 2nd molar on the posterior superior cheek. The image also shows the correct placement of the mouth brace, one rubber end on the hard palate and the other rubber end on the ipsilateral canine. Figure 2 shows an image taken after successful cannulation of the parotid papilla at the 2 cm mark on the PET10. Figure 3 shows a fluoroscopy image at the moment of a radiocontrast infusion demonstrating branching of the solution through Stensen's Duct and into the parotid gland. This fluoroscopic image was performed for the sole intention of demonstrating the anatomy and distribution of an infusate. Fluoroscopy is not required when performing this procedure for vector delivery. Figure 4 shows EGFP immunostained in red on histopathology. Both ductal and acinar cells have been stained in red, indicating successful transduction and transcription in both cell types. In summary, these four figures demonstrate appropriate RSGI with visualization of the anatomy and of transduction of Ad5 vectored EGFP.
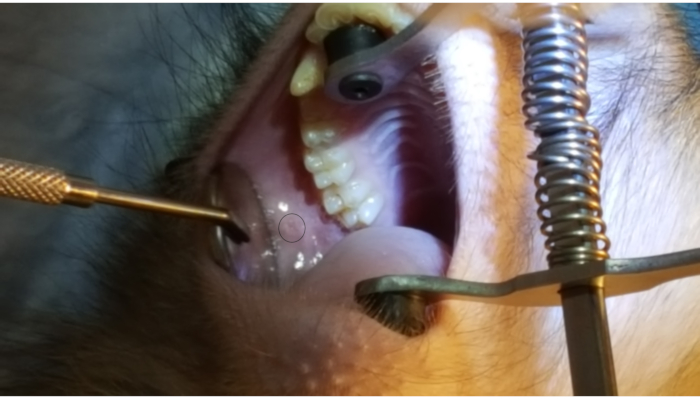
Figure 1: Parotid papilla. Note the circle on the figure highlighting the parotid papilla adjacent to the 2nd molar on the posterior cheek. Also note the placement of the mouth brace, with one rubber end on the hard palate and the other rubber band on the lower canine. Please click here to view a larger version of this figure.
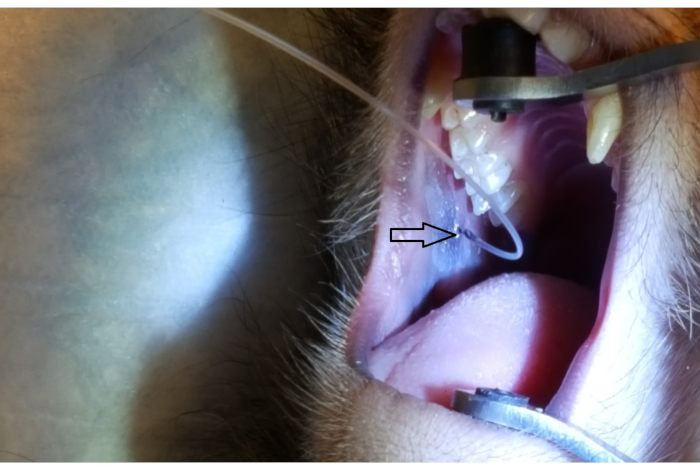
Figure 2: Parotid papilla cannulation by PET10. Note the 2 cm mark on the PET10 tube visible at the parotid papilla (arrowhead), located on the posterior cheek, adjacent to the 2nd upper molar. Please click here to view a larger version of this figure.
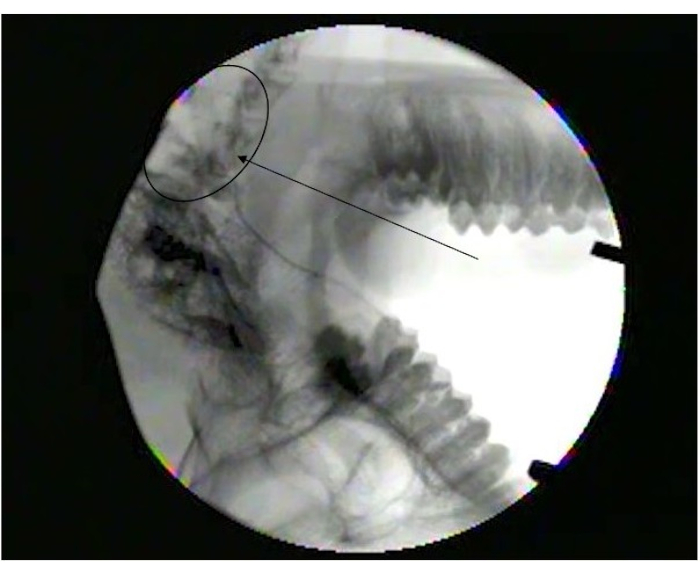
Figure 3: Fluoroscopy image showing diffusion into parotid gland. Note branching at the end of Stensen's duct (arrowhead) as it branches into smaller ducts in the parotid gland (Circle). Please click here to view a larger version of this figure.
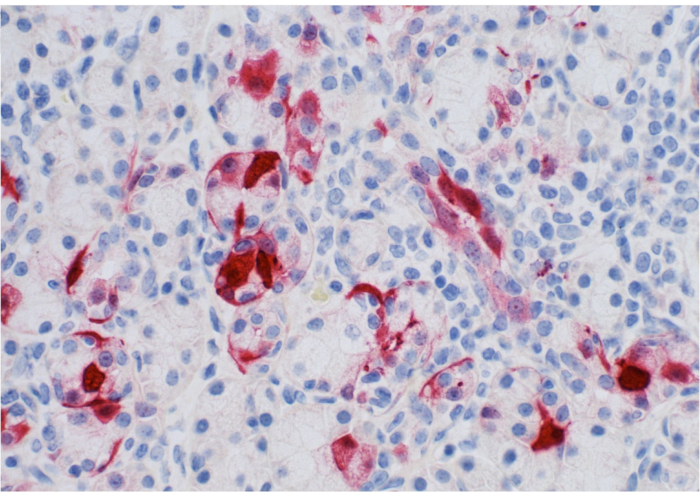
Figure 4: Pathology slide of parotid gland. Note expression of EGFP (stained in red) by ductal/acinar parotid tissue. Please click here to view a larger version of this figure.
