fNIRS was performed with hypercapnia challenge on 15 healthy participants. Exclusion criteria were history of TBI, pre-existing disabling neurological or psychiatric disorders or pregnancy. The participants had a mean age of 37.7 ± 16 years (range 20-55) and 20% were female. As shown in a similar fMRI study28, a 60 s inhalation of 5% CO2 was accompanied by an increase in EtCO2 pressure as measured by capnography. In our study, the EtCO2 trace was accompanied by an increase of HbO and a decrease of HbR (Figure 4).
Physiologically, HbO and HbR are out of phase14. In Figure 4, which represents the fNIRS signal of one participant, we observed that the HbR signal precedes the HbO signal by 3.5 s (a precise measurement can be derived from the time shift for each signal). On an average, across all participants, it was observed that the HbO signal increases 2.3+ 2.6 s after the HbR signal decreases. This implied that the time shift for HbO and HbR were different and needed to be estimated before calculating a participant’s CVR. For this same reason, we also needed to estimate the time shift between the EtCO2 tracing and Hb-diff (the difference between HbO and HbR signals). The Hb-diff parameter gave us the strongest amplitude between the two conditions.
On an average, in our HC group, the increase of HbO appeared 2.3 + 2.6 s before the HbR decrease was noted. Because of this delay between HbO and HbR, the time shift between the EtCO2 tracing and HbO signal was not the same as the time shift between the EtCO2 tracing and HbR signal. In addition, also calculated was the time shift between the EtCO2 tracing and Hb-diff (difference between HbO and HbR signal). The Hb-diff parameter gave us the strongest amplitude between the two conditions.
After shifting the EtCO2 trace for HbO, HbR, and Hb-diff, we measured the Pearson correlation between the shifted EtCO2 traces and HbO, HbR, and Hb-diff. EtCO2 trace highly correlated with fNIRS signals (Pearson’s correlations of 0.94, -0.98 and 0.91 for HbO, HbR and Hb-diff, respectively; p<0.0001). (Figure 5).
We explored the CVR inter- and intra- variability between all 15 participants and all source/detector pairs. Averaging the CVR between the source/detector pair for each participant, we assessed the CVR from HbO, HbR, and Hb-diff (difference between HBO and HbR). On average between all participants, CVR values were 13.1 + 4.7 μM/mmHg using HbO, -14.6 + 10.2 μM/mmHg using HbR, and 12.4 + 3.7 μM/mmHg using Hb-diff (Table 1). Variability between the channels within each participant was also analyzed. On average, the intra-variability of CVR assessed with Hb-diff was lowest (30%), appeared to be the best parameter to investigate CVR using fNIRS.
Finally, we can overlay the CVR values on an anatomical template or directly on the structural image of the patient’s brain, as available for better visualization.27
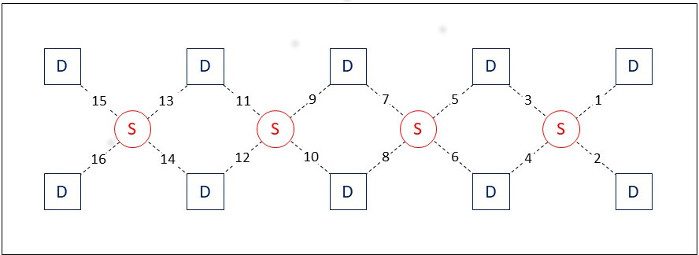
Figure 1: Optical sensor pad schematic. It is composed of 4 sources (large red circles), and 10 detectors (small red dots), which form 16 source/detector pairs having 2.5 cm separation. The sensor pad is positioned on the volunteer’s forehead. The numbers indicate the position of the 16 source/detector pairs on the sensor. Please click here to view a larger version of this figure.
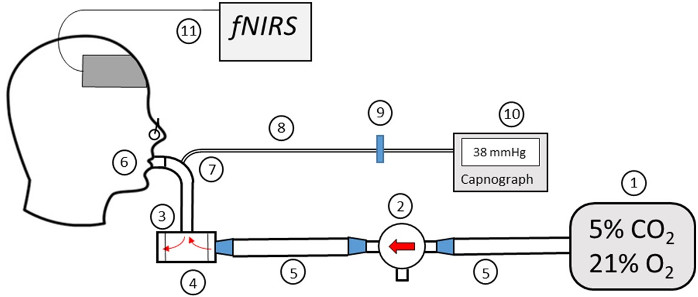
Figure 2: Diagram of the Gas Delivery System. (1) Douglas bag. (2) Three-way valve. (3) Diaphragms. (4) Two-way non-rebreathing valve. (5) Gas delivery tube. (6) Mouthpiece. (7) Connector. (8) Gas sampling tube. (9) Hydrophobic filter. (10) EtCO2 monitor. (11) fNIRS system. Please click here to view a larger version of this figure.
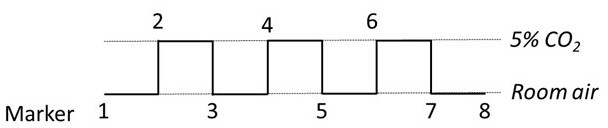
Figure 3: Timing and marker of the breathing paradigm. Every minute, the three-way valve switched between the two gases. A marker signal was sent to the fNIRS software to sort each period with the appropriate gas inhalation. Please click here to view a larger version of this figure.
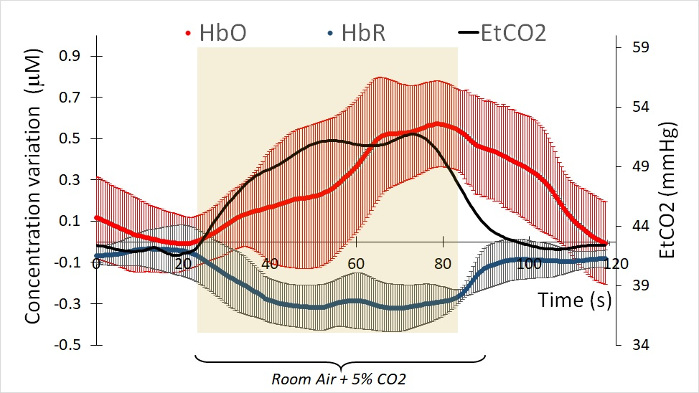
Figure 4: Example of HbO and HbR concentration measures under a 5% CO2 challenge of one participant. Each fNIRS curve is the average of 16 channels. The red curve represents the variation of HbO during 60s of room air and 60s under 5% of CO2. The blue curve represents the variation of HbR under the same conditions. The curves were time shifted in order to match the EtCO2 (black curve). Each HbO and HbR curves are the average of 3 challenges. Please click here to view a larger version of this figure.
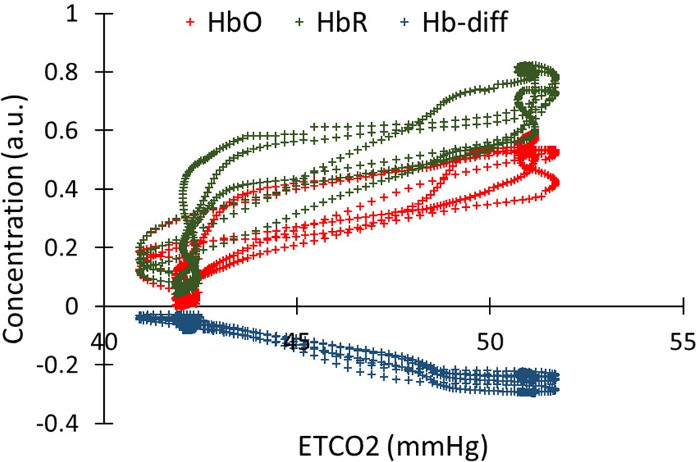
Figure 5: Correlation between the EtCO2 and the HbO, HbR, oxygenation, in one channel for one participant. HbO, HbR and oxygenation were time shifted in order to temporally match the EtCO2 trace. Pearson’s correlations is 0.94, -0.98 and 0.91 for HbO, HbR and Hb-diff, respectively (p<0.0001 ) Please click here to view a larger version of this figure.
| Mean CVR between patient | Variability between channels | |
| HbO | 13.1 +/- 4.7 | 41% |
| HbR | -14.6 +/- 10.2 | 85% |
| Hb-diff (HbO-HbR) | 12.4 +/- 3.7 | 30% |
Table 1: Inter-subject and inter-channel variability of CVR values for 15 HC. CVR variability was calculated with 3 physiological signals: HbO, HbR and oxygenation (HbO-HbR).
