Laser Speckle Perfusion Recording and Imaging: Perfusion recording was performed continuously until the animal was transported to MRI, and again at sacrifice (Figure 1A). Data showed that cerebral perfusion decreased by ~15% to 83 ± 10% at the time point before basilar artery occlusion (pre-BAO). This nominal decline is likely the result of a microcatheter insertion in the distal vertebral artery. After injecting the prepare thromboembolus, the post-BAO perfusion dropped to an average of 33 ± 2.6%, representing a ~67% decline from baseline (Figure 1B). Angiographic observation showed that blood circulation in the basilar artery was patent prior to BAO (Figure 2A) and fully occluded after administration of the autologous clot (Figure 2B). In agreement with the angiograms, laser speckle perfusion imaging (LSI) observed through the cranial window depicted unrestricted perfusion (Figure 2C) in contrast to restricted perfusion after occlusion (Figure 2D). The efficacy of embolization in the BAO model was then verified. For this purpose, the vasculature was visualized and quantified using the rt-LASCA technique15. The brain vasculatures at baseline were clearly observed (Figure 2E) while vasculature was not visualized during occlusion (Figure 2F). Mean real time perfusion (average of 10s recording) was 191.71±20.61 pu at baseline measurement and dropped to 64.71±11.35 pu (only 34% residual flow in a representative dog) at BAO. After injection of an autologous thromboembolus, the cerebellum region was immediately occluded and its territories were no longer visible during DSA analysis.
T2-weighted and FLAIR imaging: T2-weighted MRI is inadequate to detect early acute strokes (Figure 3A)18,19. This was also the case with FLAIR images (Figure 3B). T2-weighted imaging was performed to confirm whether these scans are required in the therapeutic treatment in both pre-clinical and clinical evaluations.
Figure 4. High b-value apparent diffusion coefficient (ADC) mapping enables quantification of acute ischemic stroke volume. Canine MRI was performed on five dogs. Data converted to DICOM images and transferred for post-processing. ADC maps were obtained from two sets of DWI images corresponding to the b-values of 0 and 1800 s/mm2. Representative DWI images (infarct region bright); slice1: A-B: slice2: E-F, and slice3: I-J; and respective ADC maps (infarct region dark) of three adjacent central slices, C-D, G-H, and K-L are shown. The blue color in the color images represents the low signal in the gray scale images and is the infarct region (traced with red dotted curves). (M) Quantification of infarct volume was performed by delineating the lesion borders on DICOM images using OsiriX MD v.5.0 software to calculate the areas. Area of the whole brain and infarct region so obtained were multiplied by the slice thickness (3mm) to get the brain and infarct volumes. Whole brain volume was converted as 100 percent and the infarct volume percent was calculated. Data = mean ± SEM, n=5.
Digital Subtraction Angiography and Magnetic Resonance Angiography: Magnetic Resonance Angiography (MRA) was performed using Siemens’ 3D-time-of-flight (TOF) sequence for high spatial resolution. DICOM image series were reconstructed and maximum intensity projection (MIP) was applied during post processing to visualize the blood vessels from the head and neck to confirm BAO. DSA demonstrated vascular occlusion post-BAO (Figure 5A). MRA images clearly demonstrated the restricted flow through the basilar artery as shown in representative color scale vascular image (Figure 5B).
Histological Correlation with MRI: We traced representative canine brain TTC images (Figure 6A) and MRI images (Figure 6B) to correlate infarct size and revealed a significant Pearson’s Correlation Coefficient of r=0.77 (Figure 6C).
Physiological parameters: Physiological parameters including heart rate (HR), blood pressures (BP) and temperature were monitored throughout the procedure and are critical to ensure physiological surgical procedures and proper interpretation of therapeutic and device testing (Supplementary Table 1). Representative electrocardiograms at baseline (Supplementary Figure S1A) and post-BAO before sacrifice (Supplementary Figure S1B) are shown. Laboratories who perform this model as presented should expect a significant decrease in systolic blood pressure in an acute time frame.
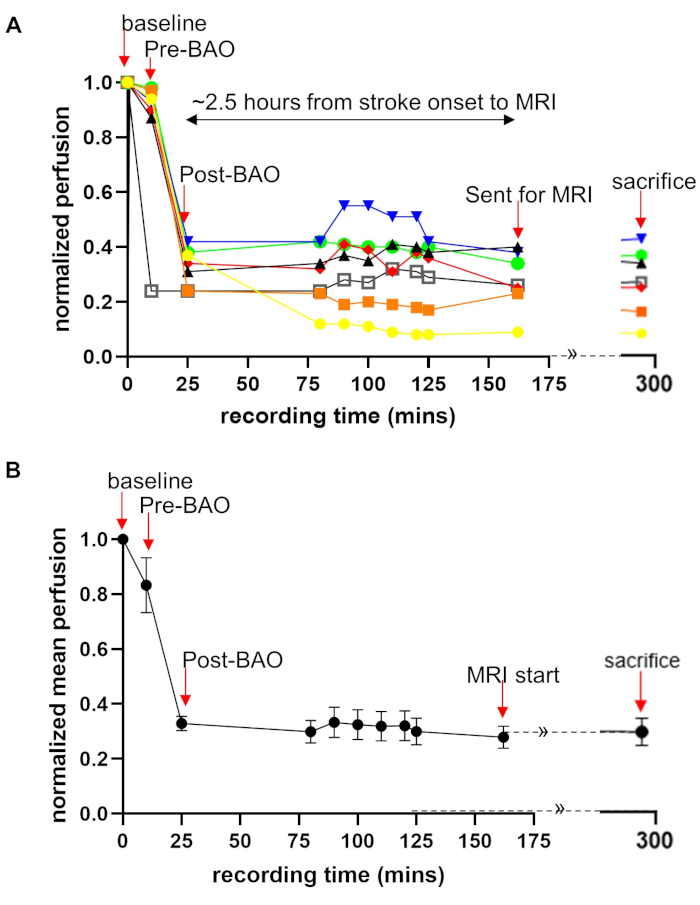
Figure 1: Quantification of laser speckle perfusion data shows restricted blood flow during and after BAO. Laser speckle perfusion recording during the experimental process performed on all seven dogs. Perfusion recording was performed for the time points: baseline, before BAO, clot placement, during onset of occlusion, throughout saline infusion (duration of stroke) after MRI exams. Data were acquired from a cranial window, providing a 1.5 cm × 1.5 cm field of view. The perfusion data were normalized as a percentage of baseline. (A) Perfusion data are shown with color line graphs for all seven dogs which showed that there is an individual difference in perfusion. (B) Mean perfusion fold change over time are shown. Data = mean ± SEM, n = 7. Arrows indicate the time points of interest. LSI data during MRI could not be collected. This part of graph is shown with dotted lines with continuation sign (»). Please click here to view a larger version of this figure.
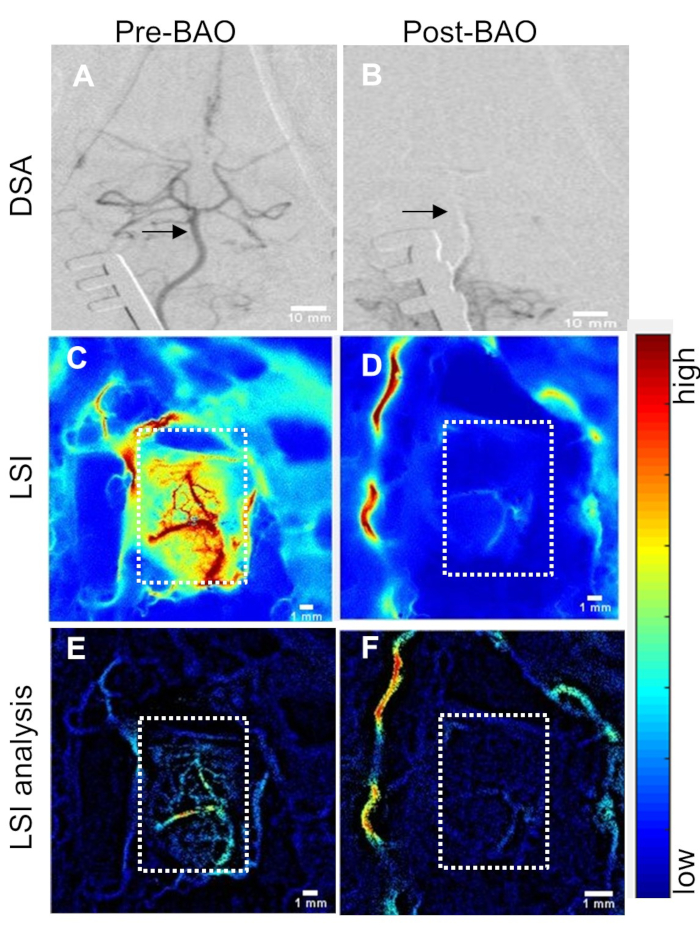
Figure 2: Cerebral perfusion measurement through cranial window correlates with changes in DSA. (A) Baseline (pre-BAO) digital subtraction angiogram (DSA) of the basilar artery and Circle of Willis. Basilar artery indicated by arrows. (B) DSA at post-BAO. (C) Laser speckle perfusion imaging (LSI) at baseline (pre-BAO) and (D) during occlusion after delivery of autologous clot. Post-processed analysis for the detection and enhancement of microvasculature using retooled laser speckle contrast analysis (rt-LASCA) technique at (E) baseline and (F) post-BAO. Color bar code: blue to red = low to high perfusion. Cranial window shown by dotted rectangles. Please click here to view a larger version of this figure.
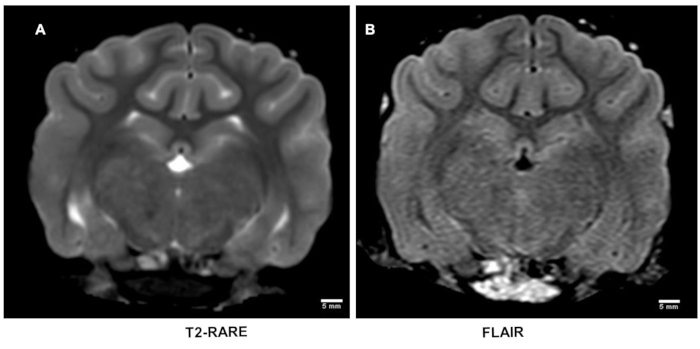
Figure 3: T2-weighted magnetic resonance imaging after stroke. T2-weighted MRI using rapid acquisition of relaxation enhancement (RARE) sequence is inadequately sensitive to detect early acute strokes (A) which was also corroborated on flow attenuated inversion recovery (FLAIR) sequence images (B). Please click here to view a larger version of this figure.
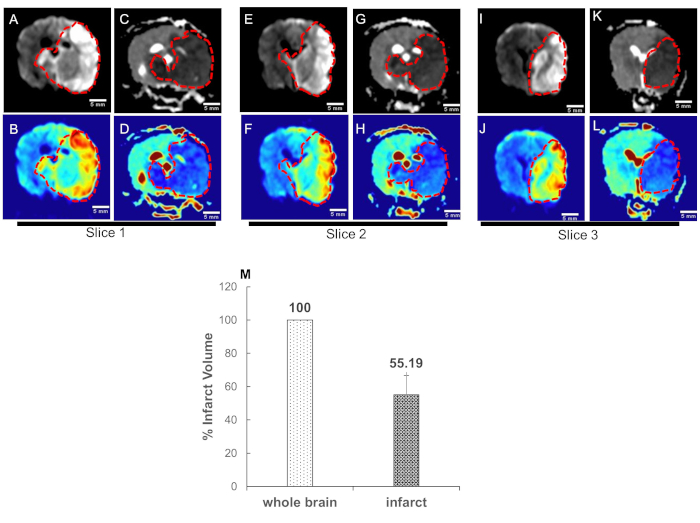
Figure 4: High b-value apparent diffusion coefficient (ADC) mapping enables quantification of acute ischemic stroke volume. Canine MRI was performed on five dogs. Data converted to DICOM images and transferred for post-processing. ADC maps were obtained from two sets of DWI images corresponding to the b-values of 0 and 1800 s/mm2. Representative DWI images (infarct region bright); slice1: A-B: slice2: E-F, and slice3: I-J; and respective ADC maps (infarct region dark) of three adjacent central slices, C-D, G-H, and K-L are shown. The blue color in the color images represents the low signal in the gray scale images and is the infarct region (traced with red dotted curves). (M) Quantification of infarct volume was performed by delineating the lesion borders on DICOM images using OsiriX MD v.5.0 software to calculate the areas. Area of the whole brain and infarct region so obtained were multiplied by the slice thickness (3mm) to get the brain and infarct volumes. Whole brain volume was converted as 100 percent and the infarct volume percent was calculated. Data = mean ± SEM, n=5. Please click here to view a larger version of this figure.
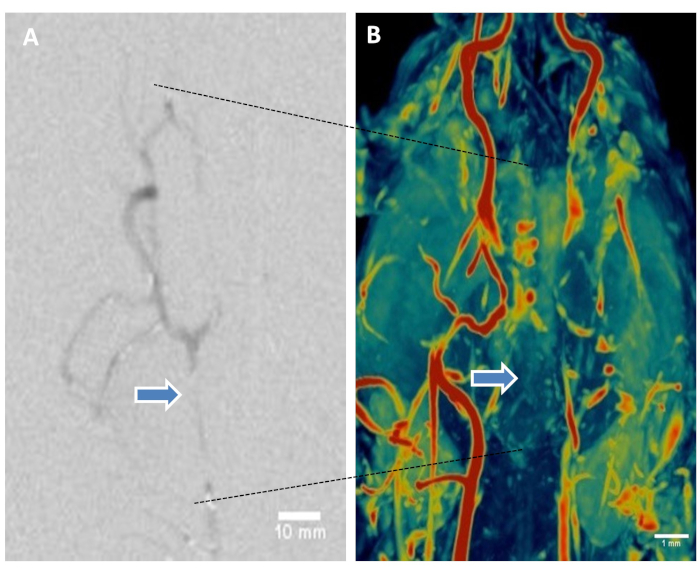
Figure 5: Digital subtraction angiography and magnetic resonance angiography of brain help visualize thromboembolic basilar artery occlusion. (A) Representative DSA showing basilar artery occlusion. (B) Representative canine brain MRA using 3D-time-of-flight sequence. Maximum intensity projection (MIP) volume rendering technique, leveling, filtering, and surface display was performed to create the MR angiograms from the DICOM image series. Color coding using color look-it-up table. Representative image shows restricted flow in basilar artery (arrows). Please click here to view a larger version of this figure.
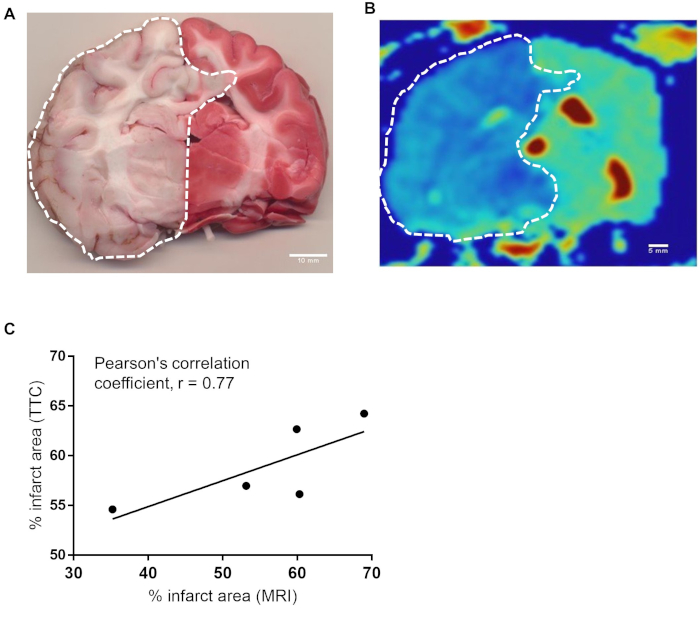
Figure 6: There is a strong correlation between infarct area of histochemical and MRI methods. (A) Representative canine brain section harvested at the time of sacrifice immediately proximal to H&E section stained with TTC 4.5 hours after BAO. (B) ADC map of corresponding brain section from MRI. Infarct area was calculated by delineating the sections of all brains stained in TTC (n=7). Similarly infarct region of one MRI slice from each brains (n=5) were delineated using OsiriX MD v.5.0 software. (C) The data were analyzed using software Prism Graph Pad 8.0. Area from TTC vs MRI were compared for Pearson’s correlation coefficient. Pearson correlation between representative TTC section and MRI section at the same location showed strong correlation, r = 0.77. Please click here to view a larger version of this figure.
Supplementary Figure S1: Physiological data before BAO and at time of sacrifice. Baseline data were compared with post-BAO in all seven dogs. Ages range from 14-21 months and body weights range from 8-13 kilograms. Mean, systole, and diastole blood pressures (BP) are shown. Representative electrocardiographs (ECGs) at baseline (A) and just before sacrifice are shown (B). Please click here to download this figure.
Supplementary Table. Please click here to download this table.
