The relevant outcomes of LARH are shown in Table 1. The patient featured in the video recovered well after the surgery and was sent back to the ward. The operation lasted 180 min, with an intraoperative blood loss of approximately 150 mL that did not require a blood transfusion. The intraoperative urinary output was 800 mL. The time for establishing the retro hepatic tunnel and transecting the liver parenchyma are 15 min and 35 min respectively. The Pringle maneuver was performed twice. The patient recovered well without postoperative complications and was discharged on the 8th postoperative day. Preoperative CT showed a moderately poorly differentiated hepatocellular carcinoma measuring 9.5 cm x 9.0 cm x 7.0 cm (Figure 1). Postoperative CT revealed complete resection of the right liver tumor, confirming R0 resection, without any significant effusion in the right liver section (Figure 8). Postoperative pathological results confirmed hepatocellular carcinoma (Figure 9). The disease-free survival (DFS) of the patient is 17 months and overall survival (OS) is 32 months.
The above case was selected to demonstrate how the surgery was performed in 82 patients. From December 2015 to June 2022, 82 patients diagnosed with large right hepatocellular carcinoma (maximum tumor diameter ≥5 cm) were recruited for the study. Overall, 54 and 28 patients underwent LARH and LCRH, respectively. LARH was performed as described above and LCRH was performed as described previously3 (see Supplementary File 1).
The perioperative clinical data and survival outcomes of the two groups were compared. The characteristics of all 82 patients are summarized in Table 2.There was no significant difference between the LARH and LCRH groups with respect to clinical characteristics (p >0.05). The surgical results are summarized in Table 3. The intraoperative blood loss, duration of the technique, liver parenchyma transection time, and complication rates in the two groups can be determined from the results. The above perioperative observation indicators demonstrate the effectiveness and safety of LARH. The intraoperative blood loss among the patients in the LARH group was less than that of the patients in the LCRH group (200 vs. 300 mL, p < 0.05). The retro hepatic tunnel was successfully established in patients who underwent LARH without massive hemorrhage, and the catheter was used to complete the hanging maneuver. The median time for establishing the retrohepatic tunnel in patients in the LARH group was 15 min. The liver parenchyma transection time among patients in the LARH group was less (p = 0.011). Furthermore, the patients in the LARH group had shorter postoperative hospital stays (8.5 vs. 11 days, p <0.05). The complication rates (grades III and IV) according to the Clavien-Dindo classification11 in the LARH group were better than those in the LCRH group (9.3% vs. 32.1%, p = 0.009). The two groups of patients successfully completed the operation, and the survival rate was 100% right after the operation.
Four of the 82 patients did not turn up for their follow-up visits and 78 patients were included in the survival analysis for a follow-up of 8-69 months, with a median follow-up of 32 months. In the LARH group, the 1, 3, and 5-year disease free survival (DFS) rates were better than those in the LCRH group (88.5% vs. 76.9%, 65.5% vs. 42.0%, 48.9% vs. 29.4%, respectively; p = 0.043)(Figure 10). The 1, 3, and 5 year OS rates were similar in the LARH group (95.5% vs. 96.2%, 70.8% vs. 64.2%, 84.5% vs. 64.2%, respectively; p = 0.35) compared to those in the LCRH group (Figure 11).The prognostic factors for OS and DFS are shown in Table 4. Multivariate analysis indicated that LARH (hazard ratio [HR]=0.518, 95% CI 0.268-1.000, p=0.049), and no vascular tumor thrombus (hazard ratio [HR]=0.110, 95% CI 0.151-0.240, p<0.001), and blood loss < 250ml (hazard ratio [HR]=2.067, 95% CI 1.027-4.163, p<0.042) were associated with longer DFS. In addition, no vascular tumor thrombus (hazard ratio [HR]=0.229, 95% CI 0.106-0.493, p<0.001) was associated with longer OS.
Table 1: Relevant outcomes of LARH. a Clavien-Dindo classification grade III/IV Please click here to download this Table.
Table 2: Patient characteristics. HBsAg, hepatitis B surface antigen; AFP, alpha-fetoprotein. Please click here to download this Table.
Table 3: Surgical results. a Clavien-Dindo classification grade III/IV Please click here to download this Table.
Table 4: Prognostic factor analysis for DFS and OS. HR: hazard ratio; OS: overall survival; DFS: disease-free survival; AFP: serum α-fetoprotein level. Data in parentheses are 95% confidence intervals. A Cox proportional hazard regression model for DFS and OS was used. Please click here to download this Table.

Figure 1: Enhanced computerized tomography confirmed a hypointense mass occupying the right liver. Please click here to view a larger version of this figure.
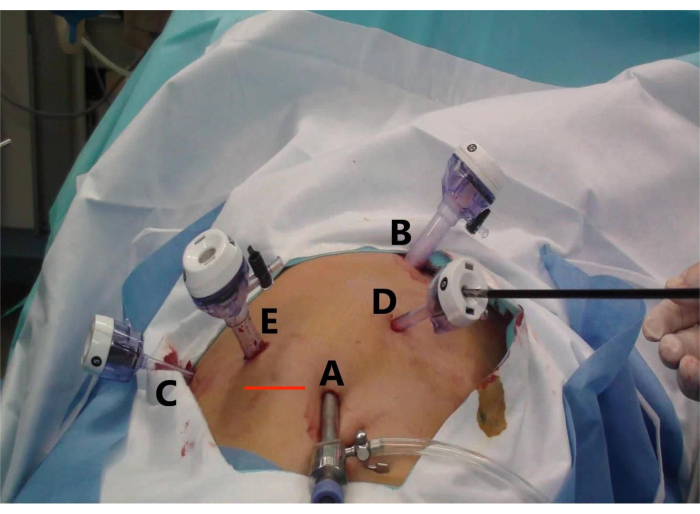
Figure 2: Trocar placement and specimen extraction incision for laparoscopic anterior right hepatectomy (LARH). The figure shows (A) the observation hole, (B) the main operation hole for the assistant, (C) the auxiliary operation hole for the operator, (D) the auxiliary operation hole for the assistant, and (E) the main operation hole for the operator, and (Line Red) the transverse incision to remove the specimen. Please click here to view a larger version of this figure.
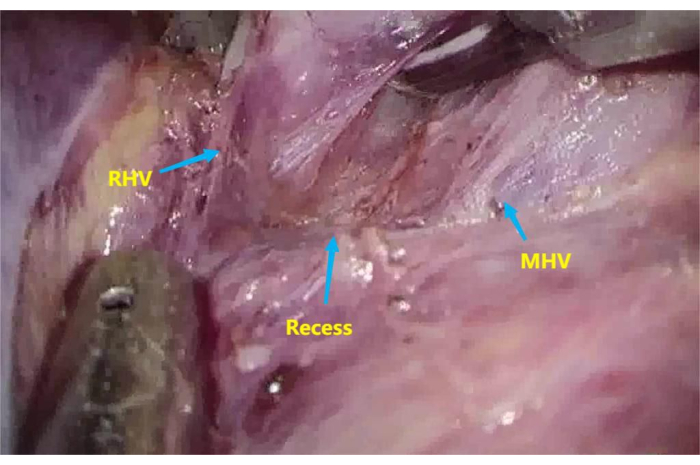
Figure 3: Recess between the root of the middle hepatic vein (MHV) and right hepatic vein (RHV). To dissect the recess between the root of MHV and RHV. Please click here to view a larger version of this figure.
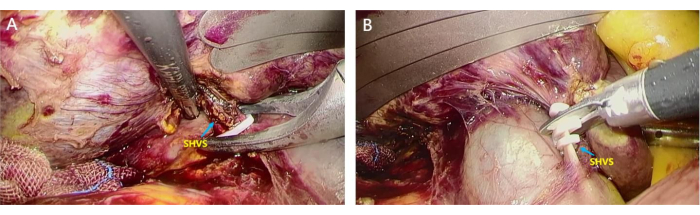
Figure 4: Dissection of short hepatic veins (SHVs). SHVs were separated and ligated to access the avascular area behind the liver. (A) The assistant lifts the liver, and the surgeon uses home-o-lock to clamp the thicker SHVSs; (B) SHVs were disconnected using a scissor to access the avascular area behind the liver. Please click here to view a larger version of this figure.

Figure 5: The use of Goldfinger dissector and urinary catheter to lift the liver. An 8-mm urinary catheter was fixed at the Goldfinger dissector, and the liver was bypassed to establish a retro hepatic tunnel. (A) The Goldfinger dissector bypassing behind the liver; (B) The insertion of the urinary catheter with a suture after the Goldfinger dissector emerged from the recess between the root of the middle hepatic vein (MHV) and right hepatic vein (RHV); (C)The urinary catheter lifting the liver after it passes through the retrohepatic tunnel. Please click here to view a larger version of this figure.
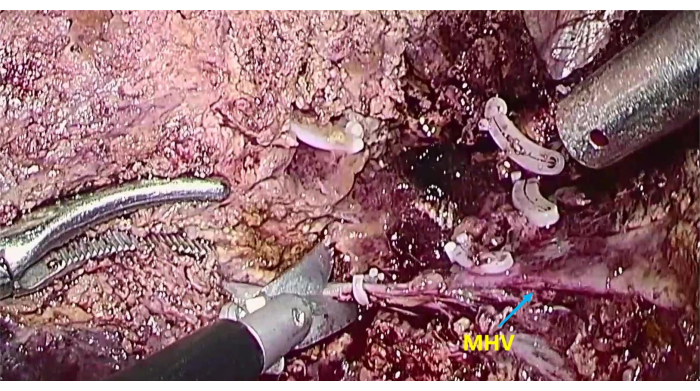
Figure 6: The exposure of middle hepatic vein (MHV) To transect the liver parenchyma along the MHV. Please click here to view a larger version of this figure.

Figure 7: The exposure of middle hepatic vein (MHV) and inferior vena cava (IVC). To expose MHV and IVC after completing liver resection. Please click here to view a larger version of this figure.

Figure 8: Postoperative enhanced computed tomography showing changes after resectioning the right hepatocellular carcinoma, suggesting a different resected right liver with indentation of an external drainage tube in the operative area compared with that observed during preoperative imaging. Please click here to view a larger version of this figure.

Figure 9: Postoperative pathological result. (A) The resected right liver tumor; (B1-3) The HE stains of the tumor confirm hepatocellular carcinoma. Please click here to view a larger version of this figure.

Figure 10: The disease-free survival (DFS) was better in the LARH group compared to those in the LCRH group, P = 0.043 (log rank test). Please click here to view a larger version of this figure.

Figure 11: The overall survival (OS) was similar in the LARH group compared to those in the LCRH group, P = 0.35 (log rank test). Please click here to view a larger version of this figure.
Supplementary File 1: LCRH steps in brief. Please click here to download this File.
