Institutional ethical approval for the protocol was obtained (ABR code: NL31401.091.10).
NOTE: The following steps describe the 3DWA protocol.
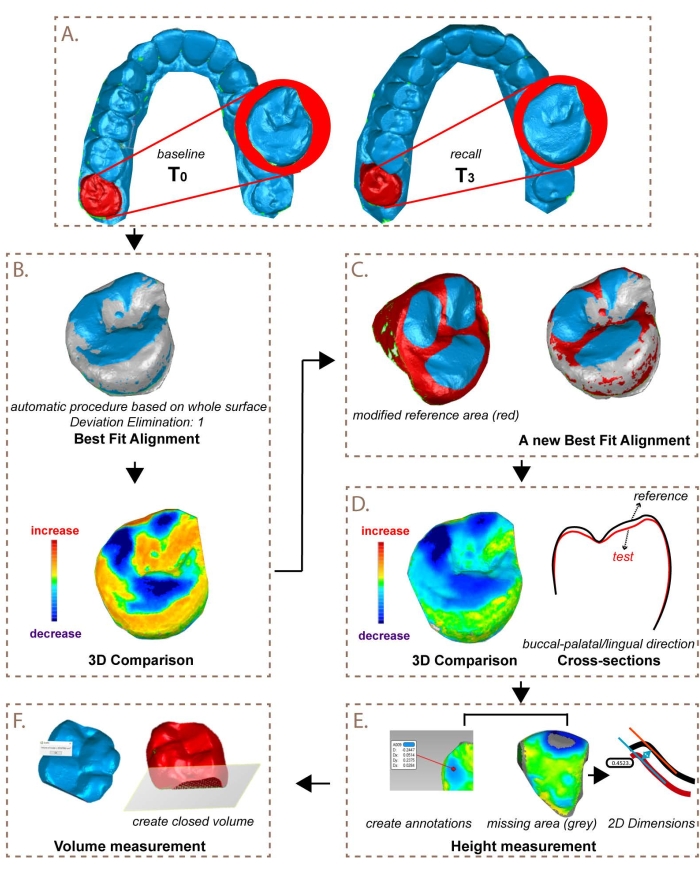
Figure 1: Visual representation of the steps for superimposition and quantitative wear measurement. This figure has been modified from K. Ning et al.23. Please click here to view a larger version of this figure.
1. Acquisition
NOTE: The following procedure was used to scan dentitions.
- Isolate the dentition using lip retractors, dry pads, and curly saliva ejectors.
- Lightly powder the dentition before scanning if required for the intra-oral scanner used.
- Scan the dentition according to the manufacturer's instructions. Refer to the Table of Materials for the products used.
2. Superimposition
NOTE: The following procedure was used for superimposition and quantitative wear measurement.
- Open the 3D software program (see Table of Materials). Open (or import) the old and new scans (STL-/PLY-file) of the upper and lower jaws.
- Select the separated teeth.
- Select a scan, and then use Lasso Selection and Select Through to select a tooth. Save the separated tooth using Tools > New Object > From Selection. Select Copy and Paste and give the object a name (e.g., 17_2016_Original).
- Repeat this procedure for each tooth of the upper and lower jaws, as well as for the old and new scans. Before selecting a new tooth, first deselect the previously selected tooth (click on the right mouse button, and then on Clear All).
- Select a specific tooth in Model Manager (e.g., 17_2016). Change Select Through with Select Visible. Use the Lasso tool to select soft tissue and contact areas and delete (right-click > Delete, or press Delete button on the keyboard) these parts. Repeat this for all individual teeth.
- Calculate best fit per tooth.
- Select in Model Manager the old scan and (by right-clicking the mouse) set this as Set Reference. Similarly, set the new scan as Set Test. Select the Reference scan and, in the Alignment tab, choose Best Fit Alignment, set Deviator Elimination 到 1, press Apply, and then OK.
- Check the quality of the best fit. Go to Analysis > Selection Through Object and create an intersection perpendicular to the surface from the buccal to the palatal side. Press on Compute. A cross-section of both scans (red and black lines) will become visible. Check if the Best Fit is correct and that the new scan is not superpositioned (higher) compared to the old scan.
- Press OK to go back to the scan.
NOTE: Optionally, the best fit might need to be improved when areas with too much wear interfere with obtaining a proper best fit. This step is described in 2.3.3.1.- Deselect areas on the old and new scans with severe material loss using the Lasso tool. Select areas on, if possible, at least three surfaces (buccal-palatinal/lingual-occlusal). Repeat step 2.3.1 through step 2.3.3.
- Select Analysis > 3D Compare to create a colorized model of the wear. In order to obtain wear facets as negative values in the results, perform the following steps.
- Change spectrum as follows: Color Segment: 21; Max. Critical: 0.2 mm; Max. Nominal: 0.02 mm; Min. Nominal: -0.02 mm; Min. Critical: -0.2 mm; Decimal Places: 3.
- Click on Apply and then OK. The result of the 3D Compare is presented in the Model Manager.
NOTE: Height decrease (wear) is shown in blue, and height increase is shown in yellow-red. Surfaces with no changes are shown in green. Surfaces the software was unable to compute due to severe loss are shown in grey. In that case, step 3.2 is followed instead of step 3.1.
3. Quantitative wear measurement: Height
- Measure the vertical height loss.
- Click on Set Result on the fitted and compared tooth. Go to Create Annotations in the Analysis tab. Change the Deviation Radius to 0.1 mm. Select the area with the largest amount of wear (darkest blue point) and click on OK to go back to the scans.
- Use Edit Spectrum to raise or decrease the value of Max Critical when the darkest blue area is too large to determine the point of highest wear. It changes the color, resulting in one clear point of darkest blue.
- Export the value from the Annotation on the point of highest wear to the data system.
- Determine the vertical material loss on 2D images with 2D Dimensions (2D Compare method).
- Set the old scan as the reference scan and the new scan as the test scan.
- Make multiple cross-sections (Analysis > Section Through Object > Compute > OK) on the locations/cusps with the largest loss of material (use the 3D Compare result to determine the location).
- Click on Test scan, and then select 2D Dimensions under the Analysis tab. In View Control, select the cross-section showing the highest height difference in the to-be-measured area.
- Select Parallels for Dimension Type.
- In the Pick Methods, click on Test. Make a mark on the Test scan at the location of the largest wear, then click on REF in the Pick Methods and make a mark on the Reference scan. Click on one selected point (highest amount of wear) to obtain the result and export this to the data system, and then click on OK.
4. Quantitative wear measurement: Volume
- Trim the teeth
- Select the tooth to be compared. Right-click on the scan and then click on Duplicate to make copies of the old and new scans of the to-be-measured tooth. Remove the automations from the copy by selecting Automations, right-clicking it, and then clicking on Delete. Select both copies of the old and new scans of the tooth.
- Go to Polygons and select Trim with Plane. Trim interdental areas and then cervical areas by creating intersections, leaving only a closed occlusal surface. Trim by drawing the intersection, resulting in a red selected area and a blue unselected area divided by the intersection.
- Click on Intersect Plane, Delete Selection, and then Close Intersection and OK to cut off the selected area on the interdental and cervical surfaces and create a closed off volume. If necessary, first reverse the selected area if the software selects the occlusal side to be deleted.
NOTE: In case the error "the intersection cannot be closed" appears, there is a hole in the chosen intersection preventing it from being closed. Slightly adjust the chosen intersection to solve this.
- Close the remaining (small) holes.
- Close small holes in the scans by selecting Fill all. Selected holes are marked with a green border, and, after filling, those will become red.
- If there are too many or too large holes preventing measurement of volume, exclude the tooth.
- Measure the volumes of both objects.
- Go to Analysis > Compute Volume. If the volume is 0, then this means that a hole is still present in the object.
- Export the values of the old and new volumes to the preferred data system.
5. Statistical analysis
- Calculate the protocol precision with a one-sample T-test, determining the structural and random error for both the height (mm) and volume (mm3).
NOTE: The random error has a zero mean and is referred to as the duplicate measurement error (DME). As the DME is present twice in repeated measurements, the DME was calculated as the standard deviation of the differences divided by √2. - Calculate the intra- and inter-precision with the paired T-test, from which the correlation, structural error, and DME are reported.
- To visualize the agreement, obtain Bland-Altman and violin plots.
- To compare and interpret results, use the trimmed ranges (P90 minus P10) calculated from the larger group of 55 patients regarding tooth wear after 0-1-, 0-3- and 0-5-year intervals for height (mm) and volume (mm3).
NOTE: These ranges were slightly trimmed to emphasize the range of more normal or less normal observations, whereas a full range would be determined by very specific observations.
During data analysis, the maximum height difference between occlusal surfaces was measured. For molars, three or four cusps were measured, and, for premolars, two cusps were measured. For maxillary anterior teeth, the incisal edge and palatal surface were measured, and, for mandibular anterior teeth, the incisal edge was measured. This resulted in a maximum of 65 measured locations per dentition. The difference in the volume of the occlusal surface was measured on posterior teeth only, resulting in a maximum of 16 observations per dentition.
Teeth with restorations on more than 75% of the measured surface were excluded, as well as third molars. On surfaces with partial restorations, height was measured on the tooth material. Height differences clearly caused by artifacts such as pooling of saliva were either excluded as a surface, or the measurement was done elsewhere on the surface. Other reasons for exclusion of surfaces or teeth were teeth being absent, the best fit being insufficient, or the data being incomplete (large gaps in the scan). Negative outcomes (inverse wear or "growth", which is clinically impossible) on included teeth and surfaces were not used for further statistical analysis except when calculating the protocol precision, for which the differences, both negative and positive, were noted.
Table 1: Results of the analysis of the precision of tooth wear measurements for height and volume. Please click here to download this Table.
Precision: structural differences
The data for protocol precision was visualized in violin plots (Figure 2 and Table 1). The data for intra- and inter-rater precision was visualized in Bland Altman plots (Figure 3 and Table 1). For height, a statistically significant difference was found between R1 and R3, which is clinically not significant, as can be seen from the entire confidence interval (ci) being close to 0. For volume, it is important to note that, for intra-rater precision, 50% of the teeth measured had to be excluded from analysis due to negative measurements (e.g., "growth") indicating inoperability.
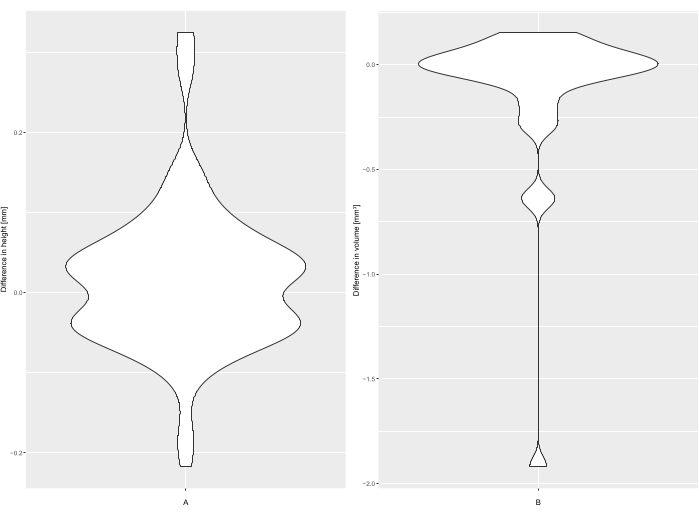
Figure 2: Violin plots for (A) height (mm) and (B) volume (mm3) for protocol precision. Please click here to view a larger version of this figure.
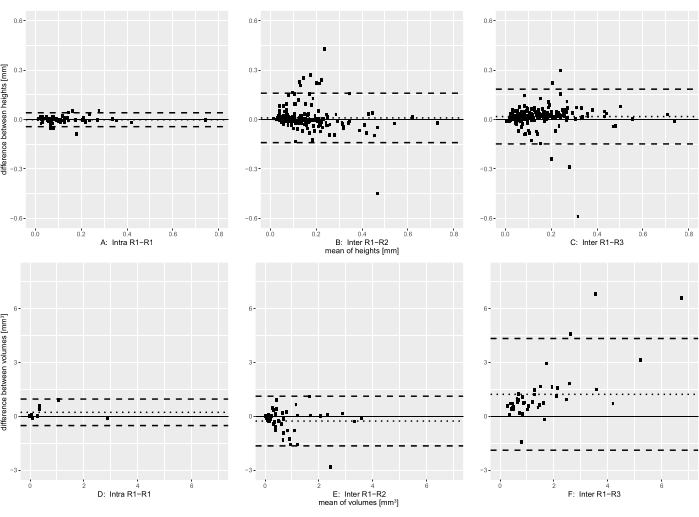
Figure 3: Bland Alman plots for (A,D) intra-rater and (B,C,E,F) inter-rater precision for height (B–C) and volume (E–F). The continued line indicates mean difference, and the dotted lines indicate limits of agreement. Please click here to view a larger version of this figure.
Precision: random error
Regarding the DME for height, there were similar DMEs for protocol precision and inter-rater precision and a much lower DME for intra-rater precision. The correlation was high and similar for inter-rater precision, very high for intra-rater precision, and could not be calculated for protocol precision. Training seemed to have little effect when looking at DME and correlation for height. Regarding volume, there were large differences between protocol precision, inter-rater precision, and intra-rater precision results.
In order to interpret the structural and random differences described in Table 1, it is important to know the range of height and volume measurements to be expected after multiple years in patients with moderate to severe wear, which are described in Table 2.
Table 2: Trimmed ranges derived from the larger group of wear patients at 0-1-, 0-3- and 0-5-year intervals and the mean difference and DME expressed in percentages of the trimmed range. Please click here to download this Table.
Interpretation of results:
Comparing the results for height to the trimmed range of wear seen in a group of 55 patients with moderate to severe tooth wear gave small structural differences (mean difference) for all intervals and all tests. For the DME, there were large differences between 0-1- and 0-3- or 0-5-intervals for all tests, indicating that, for short intervals (limited wear progression), the protocol is not precise enough, but, for longer intervals (or higher wear progression rates), the precision is adequate.
For volume, the structural differences were small on all intervals, except for the results comparing rater 1 and rater 3. For the DME, there were large differences between 0-1- and 0-3- or 0-5-intervals for all tests. Despite good results for protocol precision, there were large differences between operators, a high number of outliers, and many teeth excluded due to measured "growth", indicating poor performance of the protocol regarding volume, even for longer intervals.
The difference between protocol precision and intra-precision is due to differences in method; to calculate protocol precision, the teeth were scanned in the same session. No wear took place between the scans, resulting in an excellent best fit. Therefore, the precision of height was determined mainly by droplets of saliva and scanning powder creating tiny spikes, causing a large height difference when measuring the highest point on the surface (Figure 4). To calculate intra-rater agreement, scans were used with a 5-year interval between them, resulting in the presence of wear that increases the difficulty of performing the best fit. However, only wear was measured, and suspected saliva/powder residuals or areas with possible restorations or flaring (distortion at scanned edges of the tooth; Figure 5) were avoided, thereby increasing precision.
Since volume is calculated for the whole occlusal area and not by localized measurements, it is much less affected by occasional droplets of saliva than height when measuring protocol precision. Intra-precision would be expected to be lower than protocol precision for volume, since it is affected by the best fit procedure, which, in turn, is made more difficult by wear taking place between scans. This affects the whole occlusal area of a tooth, and, additionally, areas with saliva, powder, restorations, and flaring cannot be deselected or ignored in contrast to when height is measured. However, the results for intra-rater precision and protocol precision for volume were similar due to a single outlier decreasing protocol precision.
When analyzing the height data on wear progression comparing rater 1 to rater 2, it became clear that, for height, a group of outliers could be attributed to two factors: 1) measurements on teeth with severe wear were made with the 2D Compare method (Step 3.2), instead of 3D compare (Step 3.1), and 2) a set of measurements was wrongly made on pooled saliva, which was mistaken for wear by rater 2 (Figure 6). The data was, therefore, split into 3 groups and analyzed separately: "saliva", "normal", and "2D Compare" (Figure 6A). Rater 3 (trained) made no measurements on pooled saliva, proving that training was successful in that regard (Figure 6B).
When comparing the heights from annotations ("normal") and manual 2D measurements (2D Compare) for rater 1, the "normal" measurements had a mean height difference of 0.132 mm, with N = 223, a standard deviation of 0.112, and range: -0.001; 0.847, and the 2D Compare measurements had a mean height difference of 0.557 mm, with N = 5, a standard deviation of 0.160, and range: 0.351; 0.743, indicating that the 2D Compare measurements were in a higher range with a higher standard deviation than normal measurements
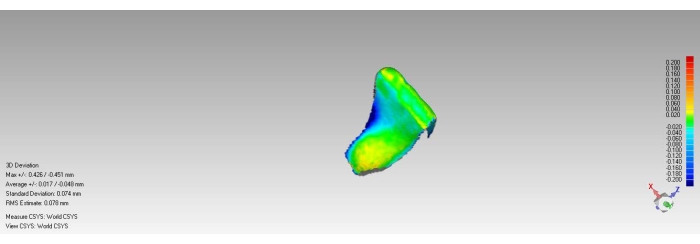
Figure 4: Example of saliva spikes on teeth without wear (incisal yellow areas) and wear caused by artifacts (lingual blue area indicating either flaring or removed calculus). Please click here to view a larger version of this figure.
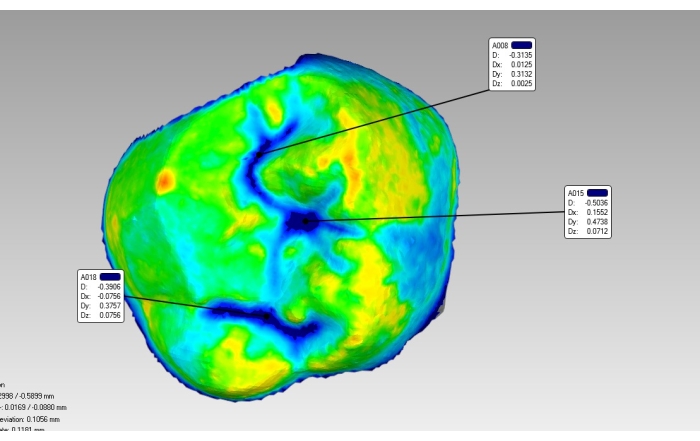
Figure 5: Example of pooled saliva in fissures (blue) and saliva spike (red-orange) on mesio-palatal and buccal cusp. Please click here to view a larger version of this figure.
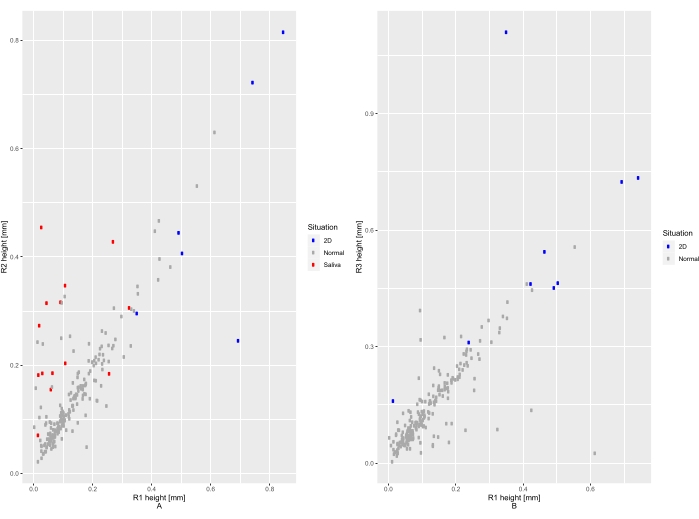
Figure 6: Scatter plots for measurement of changes in height with colored dots indicating groups of measurements ("saliva", "normal", and "2D Compare"). Please click here to view a larger version of this figure.
