Patients were selected by reviewing the records of 931 lung transplants performed at the Lung Transplantation Center of the Second Affiliated Hospital of Zhejiang University School of Medicine or the Lung Transplantation Center of Wuxi People's Hospital from 2021 to 2023. Both centers had the same surgery director leading the operating team, which comprised senior doctors and nurses with extensive experience. All donor organs were allocated fairly from the COPO system according to the principles of organ allocation and scoring.
Primary diseases of the recipients included idiopathic pulmonary fibrosis, connective tissue disease-associated interstitial lung disease, bronchiolitis obliterans syndrome, and chronic obstructive pulmonary disease. A total of 71 patients required donor lung atrial cuff reconstruction, of whom 13 received a single-lung transplant and 58 received a double-lung transplant, reflecting an incidence rate of 6.2% for atrial cuff reconstruction in double-lung transplantation. Among the 58 double-lung transplant recipients included in this study, 23 underwent posterior wall anterior rotation atrial cuff reconstruction (the preferred technique, group 1: posterior atrial flap group) and 35 underwent traditional patch reconstruction. In cases of patch reconstruction; the surgeon determined the most suitable patch material according to the condition of the donor lung. The donor aorta was used in 20 patients (group 2: aortic patch group) and the donor pericardium was used in the remaining 15 patients (group 3: pericardial patch group) Baseline characteristics of the donors and recipients are summarized in Table 1; no significant differences were observed among the groups.
Case of posterior atrial flap rotating left atrial cuff reconstruction
In October 2023, a 17-year-old male (height, 165 cm; weight, 50 kg) was admitted to the hospital because of a cough with sputum persisting for 6 months and aggravated by asthma for 3 months. Six years prior to admission, the patient developed a cough with large amounts of yellow pus sputum, which was diagnosed as bronchiectasis with infection; however, anti-infection treatment was not effective. Genetic testing revealed pulmonary cystic fibrosis. Three months prior to admission, the patient caught a cold and developed asthma, requiring continuous oxygen therapy. After treatment and discharge, but with continuous oxygen therapy at home, the activity endurance of the patient decreased significantly, and a comprehensive assessment identified indications for lung transplantation; the patient was therefore added to the waiting list. After 46 days on the waiting list, a suitable donor was identified.
The donor was a 20-year-old male (height, 170 cm; weight, 60 kg) admitted to the hospital in November 2023 with a traumatic brain injury due to a car accident. The ratio of partial pressure of oxygen in arterial blood to the fraction of inspiratory oxygen concentration was 450 and chest imaging findings were normal. The patient was pronounced brain dead on the fifth day after admission. Family members agreed to organ donation in accordance with the patient's wishes and the lungs were assessed for suitability. After cardiopulmonary intubation perfusion, the entire cardiopulmonary system was isolated, and the heart and lungs were separated in vitro. During the separation of the left atrium, the allowance of sufficient anterior wall tissue to the donor heart resulted in a defect in the atrial cuff anterior wall in the right donor lung (Figure 1B).
The double-lung transplant procedure was performed on November 23, 2023. Single-lung ventilation of the recipient resulted in stable oxygen circulation, and lung transplantation was therefore performed without extracorporeal membrane oxygenation support. During surgery, the posterior wall of the right pulmonary atrial cuff was reconstructed using the posterior atrial flap rotating left cuff reconstruction technique. The left pulmonary vein atrial cuff anastomosis was normal. The anastomosis time for the right and left pulmonary atrial cuffs was 24 min and 16 min, respectively. After all the anastomoses were completed, blood flow was restored and normal double-lung ventilation was performed. Transesophageal ultrasonography indicated a normal bilateral atrial cuff anastomotic flow rate (<140 cm/s) (Figure 4). No primary graft dysfunction (PGD) occurred and the recipient was discharged from the hospital 20 days after the lung transplantation. To date, the recipient has recovered well, with a significantly improved quality of life following the surgery.
Comparison of atrial cuff anastomosis time for 56 patients
Among the 56 patients who underwent right atrial cuff reconstruction, 23 underwent posterior atrial flap rotating left atrial cuff reconstruction and 33 underwent patch reconstruction, 20 with an aortic patch and 13 with a pericardial patch. The right atrial cuff anastomosis time was 20.5 ± 1.99 min, 22.8 ± 5.2 min, and 23.3 ± 5.3 min in the posterior atrial flap, aortic patch, and pericardial patch groups, respectively. Analysis with the Kruskal-Wallis test revealed that the anastomosis time of the posterior atrial flap was significantly shorter than that of the aortic and pericardial patches (P < 0.01); however, there was no significant difference between aortic and pericardial patching.
Among the 54 patients with right-side reconstruction and no left-side reconstruction, 21 underwent posterior atrial flap rotating left atrial cuff reconstruction, and 33 underwent aortic patch reconstruction-20 with an aortic patch and 13 with a pericardial patch. The unrepaired left atrial cuff anastomosis time was 17.5 ± 2.8 min, 17.7 ± 3.8 min, and 17.6 ± 4.3 min in the posterior atrial flap, aortic patch, and pericardial patch groups, respectively. The Kruskal-Wallis test revealed no statistically significant differences among the groups (Figure 5).
Comparison of the incidence of re-reconstruction after blood flow restoration
Anastomotic hemorrhage requiring re-reconstruction after blood flow restoration occurred in two patients (8.6%) who underwent posterior atrial flap rotating left atrial cuff reconstruction, three (15.0%) who underwent aortic patch reconstruction, and three (20.0%) who underwent pericardial patch reconstruction. Despite the lower incidence of re-reconstruction following posterior atrial flap rotating left atrial cuff reconstruction, analysis using the chi-squared test revealed no significant difference among the groups (χ2 = 0.808, P = 0.667).
Comparison of outflow velocity
Outflow velocity, as measured by esophageal ultrasound (Figure 6), revealed that patients in all three groups had normal pulmonary vein outflow channels, with no significant differences in flow rate among the groups either for the right (posterior atrial flap rotating left atrial cuff reconstruction, 53.94 ± 16.3 cm/s; aortic patch reconstruction, 60.0 ± 21.5 cm/s; pericardial patch reconstruction, 56.4 ± 17.9 cm/s; P > 0.05) or left (posterior atrial flap rotating left atrial cuff reconstruction, 64.8 ± 18.1 cm/s; aortic patch reconstruction, 68.8 ± 19.8 cm/s; pericardial patch reconstruction, 59.5 ± 16.8 cm/s; P > 0.05) pulmonary vein (Figure 7).
Comparison of cardiac ultrasonography 30 days postoperatively
Preoperative and postoperative cardiac color Doppler ultrasonography results showed no statistically significant differences in preoperative or postoperative pulmonary systolic blood pressure among the three groups (P > 0.05) (Figure 8). However, postoperative pulmonary artery systolic blood pressure was significantly lower than preoperative pulmonary artery systolic blood pressure in all three groups (posterior atrial flap rotating left atrial cuff reconstruction, 24.5 ± 7.5 vs 41.4 ± 16.6 mmHg, P < 0.01; aortic patch reconstruction, 27.6 ± 8.6 vs 35.2 ± 11.1 mmHg, P < 0.05; pericardial patch reconstruction 27.7 ± 7.5 vs 35.9 ± 14.6 mmHg, P < 0.05).
Comparison of postoperative PGD and perioperative survival
A higher incidence of PGD was observed in the posterior atrial flap rotating left atrial cuff reconstruction group (8.6%) than in the aortic (5.0%) or pericardial (13.3%) patch reconstruction groups; however, this difference was not statistically significant (χ2 = 0.431, P = 0.806). Four patients died in the perioperative period, one of whom underwent posterior atrial flap rotating left atrial cuff reconstruction, while three underwent aortic patch reconstruction (χ2 = 2.515, P = 0.284).
Comparison of clinical data 90 days postoperatively
At 90 days postoperatively, there were no significant differences in the relevant clinical characteristics among the groups (Table 2). Pulmonary function, as measured by forced expiratory volume/forced vital capacity and arterial blood gases, was significantly improved 90 days postoperatively compared to preoperatively; however, there were no significant differences in this improvement among the three groups (Table 1 and Table2).
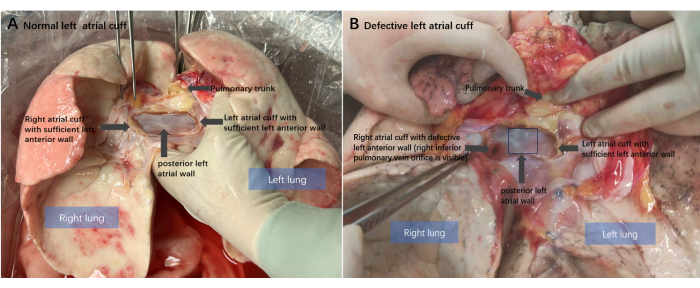
Figure 1: Anatomical diagram of the donor lung. (A) Normal left atrial cuff condition of the donor lung after heart-lung separation. The intact posterior left atrial posterior wall and sufficient anterior wall preserved. (B) The classical donor left atrial cuff anterior wall defect: the anterior atrial wall of the right donor lung is missing. Please click here to view a larger version of this figure.
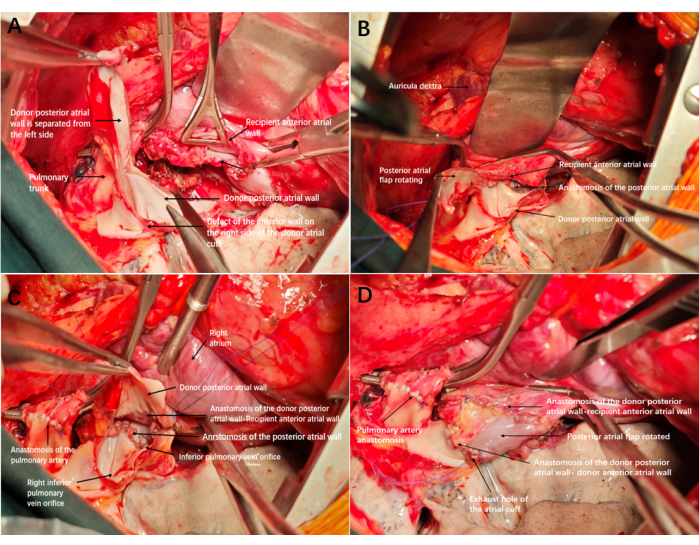
Figure 2: Reconstruction and anastomosis diagram of the left atrial cuff. (A) Defect of the anterior wall on the right side of the donor atrial cuff; after anastomosis of the trachea and artery is completed, the excess posterior wall of the atrium is cut from the bottom up to form an atrial flap. (B) Completing the anastomosis of the posterior atrial wall. (C) The edge of the atrial flap was anastomosed to the anterior wall of the recipient's atrial cuff, with the inner membrane of the atrial flap facing inward. (D) The remaining edge of the atrial cuff was anastomosed to the anterior wall of the recipient. After tightening and opening the exhaust, the cuff expanded well, with no bleeding and no need for re-reconstruction. Please click here to view a larger version of this figure.
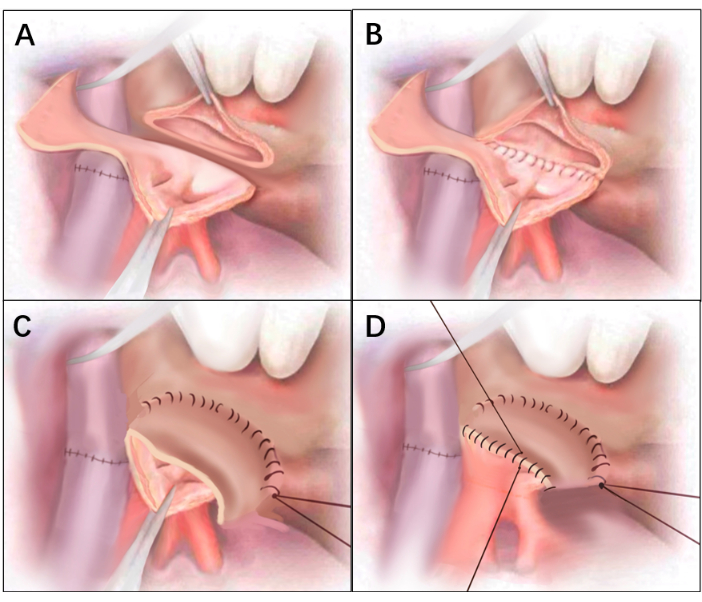
Figure 3: Line drawings of Figure 2. (A) Defect of the anterior wall on the right side of the donor atrial cuff. After anastomosis of the trachea and artery is completed, the excess posterior wall of the atrium is cut from the bottom up to form an atrial flap. (B) Completing the anastomosis of the posterior atrial wall. (C) The edge of the atrial flap was anastomosed to the anterior wall of the recipient's atrial cuff, with the inner membrane of the atrial flap facing inward. (D) The remaining edge of the atrial cuff was anastomosed to the anterior wall of the recipient. Please click here to view a larger version of this figure.

Figure 4: Esophageal ultrasonography of the bilateral atrial anastomotic flow rate. Transesophageal ultrasound images were acquired in the operating room after all anastomosis was completed, showing that bilateral atrial anastomotic flow rate was normal. Please click here to view a larger version of this figure.
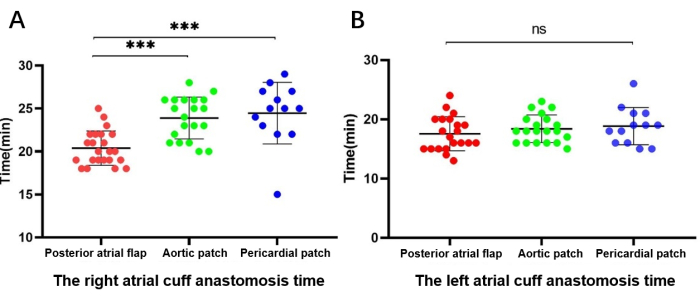
Figure 5: Comparison of the duration of atrial cuff anastomosis. (A) Right-side (reconstruction) atrial cuff anastomosis time. (B) Left-side (unreconstructed) atrial cuff anastomosis time. Please click here to view a larger version of this figure.
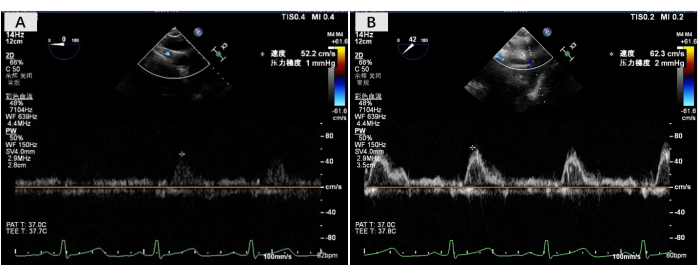
Figure 6: Esophageal ultrasonography of bilateral outflow flow rate. (A) Flow velocity measurement at the right pulmonary atrial anastomosis. (B) Flow velocity measurement at the left pulmonary atrial anastomosis. Please click here to view a larger version of this figure.
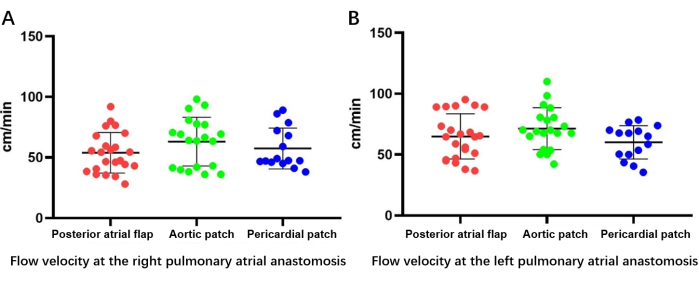
Figure 7: Bilateral outflow velocity as determined by esophageal ultrasonography. (A) Flow velocity measurement at the right pulmonary atrial anastomosis. (B) Flow velocity measurement at the left pulmonary atrial anastomosis. Please click here to view a larger version of this figure.
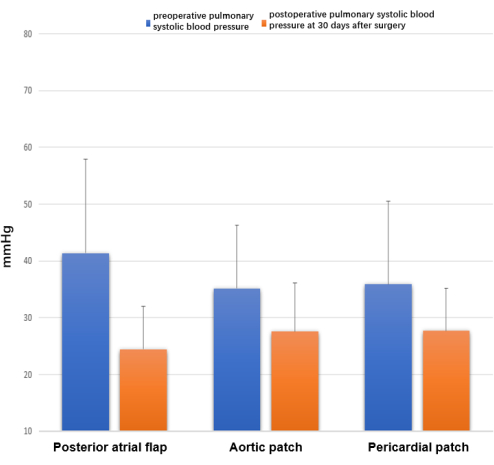
Figure 8: Echocardiography at 30 days after surgery. Differences were observed in preoperative and postoperative pulmonary systolic blood pressure, measured as 4V²TR + RPA mmHg. Please click here to view a larger version of this figure.
| Characteristic | Technique used for cuff reconstruction | P-value | ||
| Posterior atrial flap (N = 23) | Aortic patch (N = 20) | Pericardial patch (N = 15) | ||
| Donor | ||||
| Sex (F/M) | 5/18 | 4/16 | 4/11 | ns |
| Age (years) | 35.0 ± 12.9 | 36.1± 12.1 | 36.7± 10.9 | 0.86 |
| Arterial PO2/FiO2 | 401 ± 102 | 422± 106 | 426 ± 101 | 0.14 |
| Recipient | ||||
| Sex (F/M) | 2/21 | 4/16 | 6/9 | – |
| Age (years) | 47.3 ± 21.0 | 52.3± 16.2 | 49.5 ± 21.4 | ns |
| PO2 (mmHg) | 91.6 ± 21.6 | 106.7±38.3 | 102.2±35.2 | ns |
| PCO2 (mmHg) | 55.2 ± 21.7 | 54.6 ± 17.3 | 47.4 ± 11.2 | ns |
| SatO2 (%) | 96.6 ± 2.1 | 92.9± 20.3 | 91.9 ± 17.3 | ns |
| FEV1/FVC | 49.4 ± 23.9 | 48.7± 30.0 | 63.7 ± 26.0 | ns |
| PAP (cm/s) | 38.8 ± 17.9 | 44.4± 23.0 | 39.1 ± 24.4 | ns |
Table 1: Baseline characteristics of lung transplant donors and recipients. Values are presented as mean ± standard deviation. The Kruskal-Wallis test was used to compare the groups. Abbreviations: F = female; FEV1 = forced expiratory volume; FiO2 = fraction of inspired oxygen; FVC = forced vital capacity; M = male; PAP = pulmonary artery pressure; PCO2 = partial pressure of carbon dioxide; PO2 = partial pressure of oxygen; SatO2 = oxygen saturation.
| Characteristic | Technique used for cuff reconstruction | P-value | ||
| Posterior atrial flap (N = 23) | Aortic patch (N = 20) | Pericardial patch (N = 15) | ||
| PO2 | 113.2 ± 24.1 | 97.3 ± 27.5 | 98.8 ± 27.0 | ns |
| PCO2 | 40.4 ± 5.7 | 39.2 ± 10.8 | 36.4 ± 7.2 | ns |
| SatO2 | 98.1 ± 0.9 | 93.0 ± 21.1 | 93.7 ± 16.7 | ns |
| FEV1/FVC | 86.1 ± 10.3 | 87.1 ± 19.4 | 81.9 ± 17.6 | ns |
Table 2: Clinical characteristics of lung transplant recipients 90 days postoperatively. Values are presented as mean ± standard deviation. The Kruskal-Wallis test was used to compare the groups. Abbreviations: FEV1 = forced expiratory volume; FVC = forced vital capacity; PCO2 = partial pressure of carbon dioxide; PO2 = partial pressure of oxygen; SatO2 = oxygen saturation.
