Evaluating the number of apoptotic cells detected by TUNEL staining, the levels of inflammatory markers (detected in the perfusate using the QAH-INF-1 assay kit), and the general physical appearance (Stained with hematoxylin and eosin (H&E)) of heart-beating donor lungs in all groups is necessary to determine how well EVLP preserved DCD donor lungs. All DCD donor lungs underwent 4 h of perfusion. Most lungs exhibited stable compliance, with a gradual decrease observed over the 4 h period (Figure 5B). No significant differences were found in vascular resistance and pulmonary graft oxygenation levels among the DCD donor lungs (Figure 5A,C). Glucose levels in the perfusate declined over time, with no significant differences observed between individual rats (Figure 5D). Electrolyte levels in the perfusate remained similar across groups (Figure 5E-F).
TUNEL staining was performed using the terminal deoxynucleotidyl transferase dUTP nick end labeling technique with the apoptosis detection kit, following the manufacturer's instructions for apoptotic nuclear detection. TUNEL staining was employed to quantify apoptosis (programmed cell death) of alveolar epithelial cells in DCD donor lungs under different preservation conditions. Blinded analysis of apoptotic cell numbers revealed a significantly higher number of positive cells in the donor group compared to other groups. Additionally, the cold preservation group exhibited a higher number of positive cells compared to the EVLP-perfused DCD donor lungs (Figure 6). Five independent variables were used to score the pathological sections stained by H&E: 1) inflammatory cell influx in alveolar space, 2) alveolar septal thickening, 3) intra- and extra-alveolar hemorrhage, 4) intra-alveolar edema, and 5) hyaline membrane formation. Variables were scored from 0-4:0 = negative, 1 = slight, 2 = moderate, 3 = high and 4 = severe. The sum of the scored variables generated the total lung injury scores. The Lung injury score is significantly lower in the EVLP group than in the cold static preservation group and the control group (Figure 7A). Alveolar wall thickening and alveolar hemorrhage can be observed in the 4 h cold static preservation group (Figure 7B). The normal alveolar structure is maintained in the EVLP group (Figure 7C).
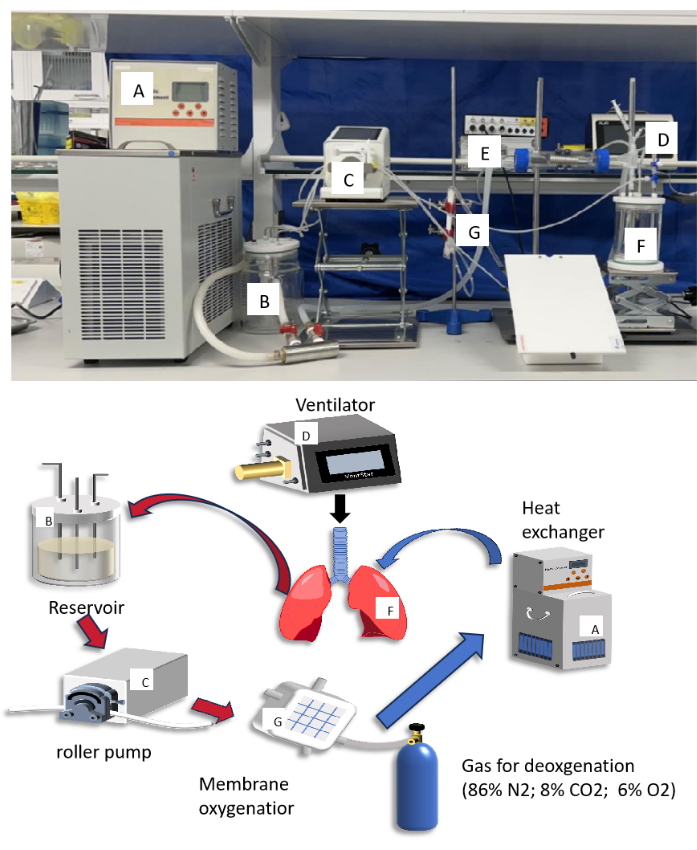
Figure 1: Diagram and photograph of small animal ex vivo lung perfusion (EVLP) circuit. The letters in the diagram matched up with the letters in the photograph to describe what each component does. Please click here to view a larger version of this figure.
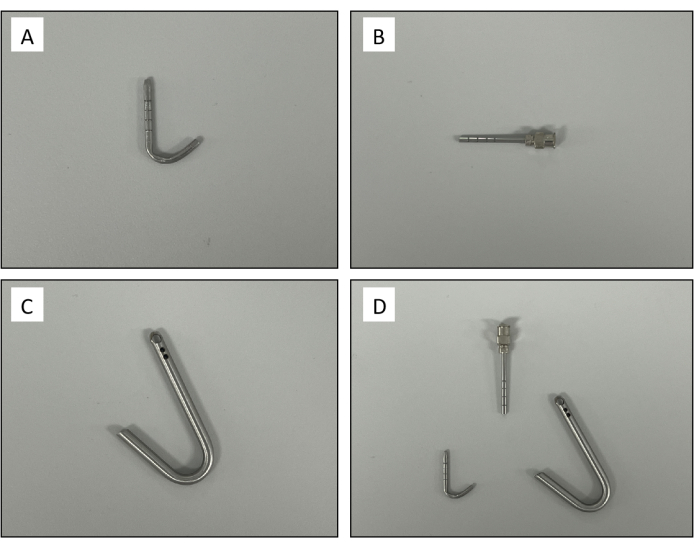
Figure 2: Custom-made cannulas. (A) Pulmonary artery cannula. (B) Trachea cannula. (C) Left atrium cannula. (D) A set of rat ex vivo lung perfusion cannula. Please click here to view a larger version of this figure.
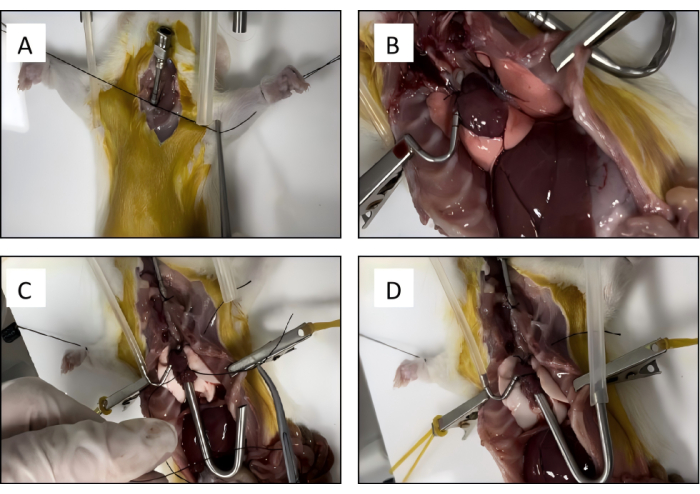
Figure 3: Rat lung isolation. (A) The trachea cannula is placed into position and secured with a silk suture. (B) The pulmonary artery is cannulated and tied with the previously placed silk suture. (C) The left atrium cannula is secured with a silk suture. (D) The connective tissue is bluntly dissected to remove the heart-lung block. Please click here to view a larger version of this figure.
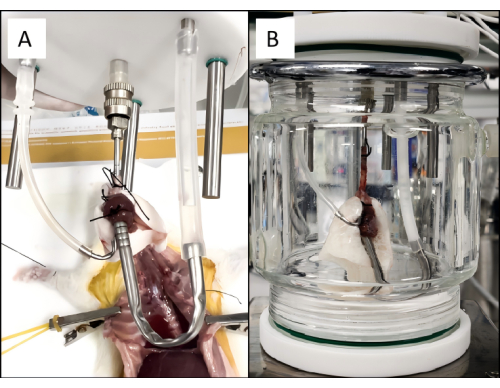
Figure 4: Rat pulmonary perfusion setup. (A) The heart-lung block is placed into the ex vivo lung perfusion circuit. (B) A properly ventilating and perfusing lung connected to the EVLP circuit. Please click here to view a larger version of this figure.
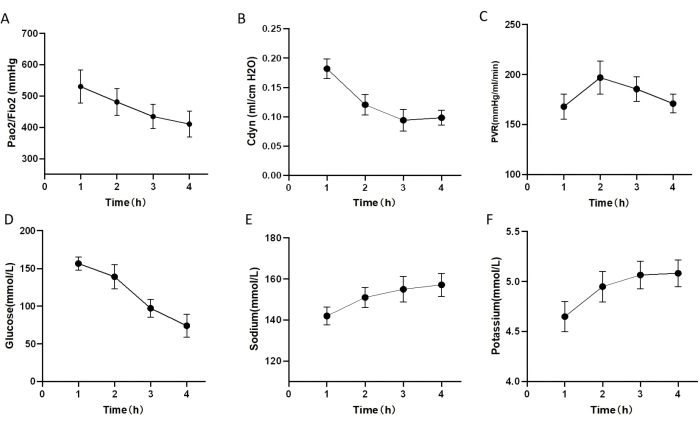
Figure 5: Lung function during rat EVLP protocol. (A-F) Lung function and blood gas analysis of donor lungs undergoing EVLP after exposure to 1 h warm ischemic time (WIT). (A) Pulmonary oxygenation index. (B) Dynamic lung compliance (Cdyn). (C) pulmonary vascular resistance (PVR). (D) The glucose level in perfusion 4 h after EVLP. (E) The sodium level in perfusion 4 h after EVLP. (F) Potassium level in perfusion 4 h after EVLP. The error bars indicate standard deviation. Please click here to view a larger version of this figure.

Figure 6: Representative images of TUNEL assay of different cases. TUNEL-positive cells: Green fluorescence shows apoptotic cells, DAPI: Blue fluorescence represents the nucleus, Merge: All cells, including cells undergoing programmed cell death (apoptosis); DCD refers to the group of direct lung harvest. DCD+COLD refers to the group of 4 h cold static preservation. DCD+EVLP refers to the group of 4 h ex vivo lung perfusion (EVLP). Please click here to view a larger version of this figure.

Figure 7: Lung injury score and histological findings. (A) The Lung Injury Score in the control group, SCS, and EVLP group (*, p <0.05). (B) Representative hematoxylin and eosin (H&E) stained slices of cold static preservation (SCS) donors. The black arrow indicates rupture of the pulmonary capillary epithelium, and the blue arrows indicate thickening of the alveolar walls. (C) Representative H&E-stained slices of EVLP donors. The red arrow indicates infiltration of inflammatory cells. (D) Representative H&E-stained slices of direct harvest donors (control). The black arrows indicate rupture and bleeding of pulmonary capillary epithelium. The error bars indicate standard deviation, significance analysis was performed by one-way analysis of variance (ANOVA). Please click here to view a larger version of this figure.
