Figure 1A shows the time course of dye injection in relation to the onset of BSW, with a peak overpressure of 25 kPa. In the 'Post' protocol, Evans blue solution was administered intravascularly 2 h before FITC-dextran perfusion, which was conducted 6 h, 1 day, 3 days, and 7 days after BSW exposure. In the 'Pre' protocol, Evans blue solution was injected immediately before BSW exposure. In the 'Post' protocol, the concentration of Evans blue is expected to reach its maximum approximately 2 h before perfusion fixation, whereas in the 'Pre' protocol, it is expected to reach its maximum around the time of BSW exposure (Figure 1B). The concentration of FITC-dextran in the brain-blood vessels was maintained constant for 2 min during perfusion.
Evans blue labeling showed that BBB breakdown started within 6 h and continued until 7 days after BSW exposure (Figure 2A). Notably, BBB breakdown did not occur immediately after BSW exposure, as there was no Evans blue dye extravasation at 3 h in the 'Pre' protocol (Figure 2B). Surprisingly, long-term labeling with Evans blue indicated its cumulative nature in the 'Pre' protocol (Figure 2B)7.
The use of two distinct dyes, each introduced at intervals of 2 h or more, allowed the examination of temporal changes in BBB integrity by comparing their distribution. Figure 3 shows fluorescence images of the slices that exhibited a significant difference in the distribution of Evans blue and FITC-dextran.
Numerous fluorescence hotspots of various sizes were observed. Although some hotspots were bright enough to rank among the top 0.1% of pixels, many were only slightly brighter than the surrounding tissues. The discrepancy between the dyes suggests that changes occurred within this interval. Hotspots displaying only Evans blue fluorescence indicated ongoing BBB breakdown at the time of Evans blue injection, which was later repaired by the FITC-dextran injection. In contrast, hotspots showing only FITC-dextran fluorescence suggested that BBB disruption occurred between the two dye injections. Lastly, hotspots exhibiting fluorescence from both dyes indicated continuous BBB breakdown during the entire injection period.
Figure 4A presents the number of hotspots positive for Evans blue (including both Evans blue-only and Evans blue/FITC-dextran double-positive hotspots), FITC-dextran (including both FITC-dextran-only and Evans blue/FITC-dextran double-positive hotspots), or both dyes (only Evans blue/FITC-dextran double-positive hotspots). In the 'Pre' protocol at 3 h, numerous FITC-dextran-only hotspots were observed. At 6 h and 1 day in the 'Post' protocol, both Evans blue-only and FITC-dextran-only hotspots were detected. However, at 3 days and 7 days in the 'Post' protocol, the hotspots were predominantly positive for both dyes. These findings suggest that BBB breakdown occurred at 3 h, was remodeled by 1 day, and persisted until 7 days after BSW exposure (Figure 4B). Importantly, the extent of BBB breakdown tended to decrease by 7 days, as previously mentioned.
Following the completion of the dye extravasation experiments, immunohistochemical staining of the slices was carried out7. The immunohistochemical image scans were consistently compared with those of the dye extravasations, confirming that the carry-over effect of the fluorescent substances was practically negligible7. As shown in Figure 5, clusters of reactive astrocytes were closely associated with sites of BBB breakdown. Further observations revealed that activated and amoeboid microglia were present alongside reactive astrocytes 3 days after BSW exposure.
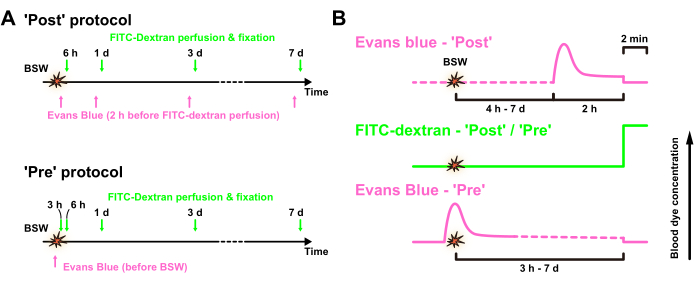
Figure 1: Experimental design. (A) Time course of the experiment. Evans blue solution was intravenously injected after ('Post' protocol) or immediately before ('Pre' protocol) BSW exposure, whereas FITC-dextran was transcardially perfused for 2 min before fixation. (B) Expected concentrations of Evans blue and FITC-dextran in the blood vessels in the 'Post' and 'Pre' protocols, respectively. BSW, blast-induced shock waves; FITC, fluorescein isothiocyanate. This figure is adapted from Nishii et al.7. Please click here to view a larger version of this figure.
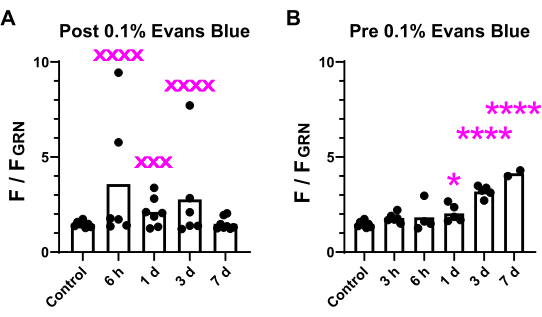
Figure 2: Comparison of fluorescence intensity in brain slices. The fluorescence intensity of the brightest 0.1% of pixels in the brain was assessed across all 12 slices and compared between the 'Post' (A) and 'Pre' (B) conditions. The variability and significance of the differences are indicated. xxx denotes p < 0.001; xxxx denotes p < 0.0001 (p values from F-test). *p < 0.05; ****p < 0.0001 (analysis of variance with Dunnett's multiple comparisons post hoc test). This figure is adapted from Nishii et al.7. Please click here to view a larger version of this figure.
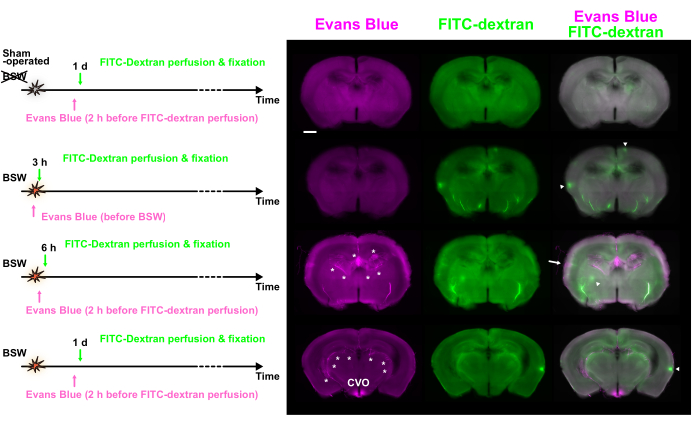
Figure 3: BBB breakdown observed at various time points using double labeling with Evans blue and FITC-dextran. Evans blue (magenta), FITC-dextran (green), and merged images are shown. The dye injection protocols are presented on the left side. Some hotspots showed predominant fluorescence of Evans blue (arrow) or FITC-dextran (arrowheads). Asterisks indicate the choroid plexus and related vessels. BBB, blood-brain barrier; FITC, fluorescein isothiocyanate; CVO, circumventricular organs of the third ventricle. Scale bar: 1 mm. This figure is adapted from Nishii et al.7. Please click here to view a larger version of this figure.
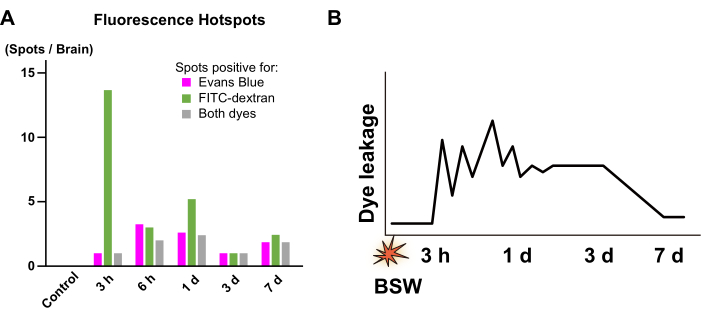
Figure 4: Quantification of the fluorescence hotspots. (A) Numbers of the hotspots positive for Evans blue (magenta), FITC-dextran (green), and both dyes (gray). They were collected from the images obtained at 3 h in the 'Pre' protocol as well as from the images obtained at 6 h, 1 day, 3 days, and 7 days in the 'Post' protocol. From 3 h to 1 day, a significant portion of the fluorescence hotspots showed a between-dye mismatch, whereas, from 3 days to 7 days, such mismatch was hardly observed. (B) Scheme summarizing the time course of BBB breakdown. The vertical axis conceptually represents the intensity of dye leakage due to BBB breakdown. The zigzag pattern from 3 h to 1 day indicates that the location and intensity of dye leakage are unstable during this period. FITC, fluorescein isothiocyanate; BBB, blood-brain barrier; BSW, blast-induced shock waves. This figure is adapted from Nishii et al.7. Please click here to view a larger version of this figure.
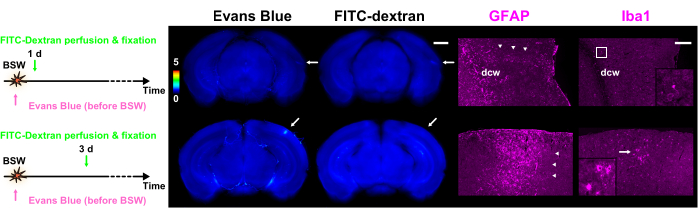
Figure 5: Expression of GFAP and Iba1 as markers for astrocytes and microglia, respectively. Each column of the figure contains fluorescence images of dye extravasation with Evans blue or FITC-dextran, along with GFAP or Iba1 immunohistochemical images. The color bar indicates normalized fluorescence intensities of Evans blue and FITC-dextran using those within GRN. The dye injection protocols are presented on the left side. The slice of 1 day in the 'Pre' protocol shows fluorescence of both Evans blue and FITC-dextran, whereas the slice of 3 days in the 'Pre' protocol shows only fluorescence of Evans blue (arrows). The regions denoted by the arrows in the dye extravasation images align with the immunohistochemical images. Arrowheads indicate clusters of reactive astrocytes. The polyclonal GFAP antibody labeled astrocytes in and around the white matter as well as in nervous tissue adjacent to the pia mater. As a result, astrocytes within and close to the dcw are labeled in this figure. The magnified images corresponding to the frame or arrow in the Iba1 column are depicted in the insets. Scale bars: 1 mm and 200 µm for the dye extravasation and immunohistochemical images, respectively. GFAP, glial fibrillary acidic protein; Iba1, ionized calcium-binding adapter molecule 1; FITC, fluorescein isothiocyanate; BSW, blast-induced shock waves; dcw, deep cerebral white matter. This figure is adapted from Nishii et al.7. Please click here to view a larger version of this figure.
